









Cystinuria: definition, causes and natural treatments
Cystinuria is an inherited defect in the tubular reabsorption of an amino acid, cystine, with increased urinary excretion of it and formation of cystine stones in the urinary tract. Symptoms may be renal colic, urinary tract infection, or kidney failure. The treatment is based on an increase in fluid intake, an adaptation of the diet, an alkalinization of the urine or even the taking of drugs to dissolve the cystine.
What is cystinuria?
Cystinuria is a rare inherited kidney disorder that causes excessive excretion of cystine in the urine. This amino acid, very poorly soluble in urine, then forms crystals, which aggregate into stones in:
- calyxes of the kidneys;
- the pyelons or pelvis, that is to say the areas where urine is collected and then evacuated out of the kidney;
- the ureters, which are the long, narrow ducts that carry urine from the kidneys to the bladder;
- the bladder ;
- urethra.
The formation of these cystine stones – or lithiasis – can lead to chronic kidney disease.
The prevalence of cystinuria varies widely by ethnicity, ranging from 1 in 2 in the Lebanese Jewish population – the population with the highest frequency – to 500 in 1 in Sweden. The overall average prevalence is estimated at 100 in 000 people. Men are generally more affected than women.
Cystinuria manifests itself at any age. Men tend to have more serious illness. The appearance of kidney stones before the age of three is more common in boys. Calculations are bilateral in over 75% of cases and recur in over 60% of cases, with greater frequency in men. Although it accounts for only 1 to 2% of adult stones, it is the most common genetic lithiasis, and is responsible for about 10% of children’s stones.
What are the causes of cystinuria?
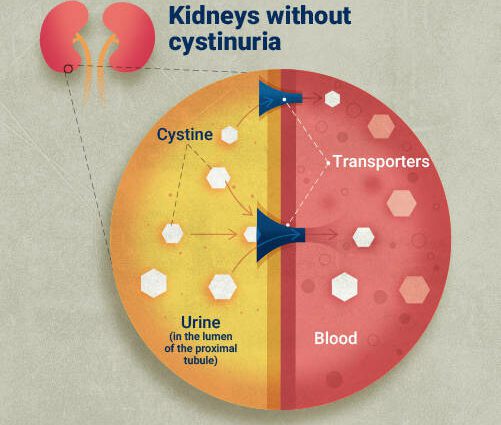
Cystinuria is caused by an inherited abnormality of the renal tubules, resulting in reduced proximal tubular renal reabsorption of cystine, and increased urinary cystine concentration.
There are two genetic abnormalities that cause most cases of cystinuria:
- homozygous mutations of the SLC3A1 gene (2p21) involved in type A cystinuria;
- homozygous mutations in the SLC7A9 gene (19q13.11) involved in type B cystinuria.
These genes encode proteins which together form a heterodimer responsible for the transport of cystine in the proximal tubule. An abnormality in either of these proteins results in transporter dysfunction.
Because these genes are recessive, people with this disease must have inherited two abnormal genes, one from each parent. A person who has only one abnormal gene may excrete more than normal amount of cystine in the urine but not enough to form cystine stones. There is no relationship between the “genotype” (cystinuria A or cystinuria B) and the precocity or severity of symptoms.
What are the symptoms of cystinuria?
Although symptoms of cystinuria can appear in infants, the first symptoms appear before the age of 20 in about 80% of patients, and on average around 12 years in girls and 15 years in boys.
Often the first symptom is an intense pain, which can go as far as the attack of “renal colic”, caused by a spasm of the ureter, at the place where the stone is locked. Urinary tract stones can also cause:
- persistent lower back or abdominal pain;
- hematuria, that is to say the presence of blood in the urine;
- elimination of small stones in the urine (especially in infants).
They can also become a site where bacteria build up and cause a urinary tract infection or, more rarely, kidney failure.
In very rare children, cystinuria may be associated with neurological abnormalities such as neonatal hypotonia, seizures, or developmental delay. These are complex syndromes due to “deletions”, that is to say the loss of a DNA fragment, carrying several genes contiguous to the SLC3A1 gene on chromosome 2.
How to treat cystinuria?
Treatment of cystinuria involves preventing the formation of cystine stones by maintaining low concentrations of this amino acid in the urine.
Increased fluid intake
For this purpose, one should drink an amount of fluid sufficient to produce at least 3 to 4 liters of urine per day. As the risk of stone formation is higher at night, because you do not drink and urine is produced in lesser quantities, it is recommended that you drink fluids before going to bed. In infants, taking drinks at night may require the installation of a nasogastric tube or a gastrostomy.
Diet low in protein and salt, and high in alkalizing foods
A diet low in methionine, a precursor of cysteine, lowers urinary cystine excretion. Methionine is an essential amino acid, so its removal is not possible but its intake may be limited. For this, it is a question of eliminating foods very rich in methionine such as dried cod, horse meat or even crayfish and gruyere, and limiting the consumption of meat, fish, eggs to 120-150 grams per day. and cheeses. The low protein diet is not recommended for children and adolescents.
Increasing the intake of alkalizing foods such as potatoes, green or colorful vegetables, and bananas, along with less salt intake can also help reduce the concentration of cystine in the urine. In fact, the urinary excretion of sodium increases that of cystine. Thus, in some patients, urinary cystine excretion may decrease by 50% by reducing dietary sodium intake to 50 mmol / day.
Drugs to alkalize urine
Since cystine dissolves more easily in alkaline, i.e. basic, urine than in acidic urine, it may be recommended, to make the urine less acidic and therefore increase the solubility of cystine, thus to take :
- alkaline waters;
- 6 to 8 grams per day of potassium citrate in 1,5 to 2 liters of water;
- 8 to 16 grams per day of potassium bicarbonate in 2 to 3 liters of water;
- or else acetazolamide 5 mg / kg (up to 250 mg) orally at bedtime.
Medicines to dissolve cystine
If stones continue to form despite these measures, the following drugs may be given:
- penicillamine (7,5 mg / kg orally 4 times / day in young children and 125 mg to 0,5 g orally 4 times / day in older children);
- tiopronin (100 to 300 mg orally 4 times / day);
- or captopril (0,3 mg / kg orally 3 times / day).
These drugs react with cystine and keep it in a form up to fifty times more soluble than cystine itself.
Urological management
The management of stones that do not go away spontaneously requires urological techniques for the treatment of lithiasis. The urologist may use the least invasive procedures, depending on each situation, such as ureterorenoscopy or percutaneous nephrolithotomy.
Doamne ajuta! am facut analise de urine si urine 24h cistina (u) e ossalato . cistina (u)= 7,14 creatinine(urine)=0,33 ; cystine (u)24h=0,020, cystine 2,44;
u-ossalat =128, 11,2 ; u-ossalat 24h= 42,8 ; 37,5 va scriu si u-sodio=24, 2800 ; u-sodio24h=48, 134
puteti sa mi dati un dagnistic. va multumesc mult de tot o seara buna.