









Contents
The scalene muscle: everything about this neck muscle
Scalene muscles are muscles in the neck, which allow it to move sideways. These three flexor muscles which are the anterior scalene muscle, the middle scalene and the posterior scalene are so named because they have the shape of a scalene triangle.
A scalene triangle is, in geometry, a triangle whose three sides are unequal. The term comes, etymologically, from the Latin “scalenus«, And further from the Greek«scaleWhich means “oblique” or “lame”, hence “odd, unequal”. These scalene muscles are stretched between the cervical processes, that is, the bony protrusions of the cervical vertebrae, and the first two pairs of ribs.
Anatomy of scalene muscles
The scalene muscles are muscles of the neck, located deep. They exhibit a scalene triangle shape, which is, in geometry, a triangle with three unequal sides. The term comes, etymologically, from the Latin “scalenus«, And further from the Greek«scaleWhich means “oblique”.
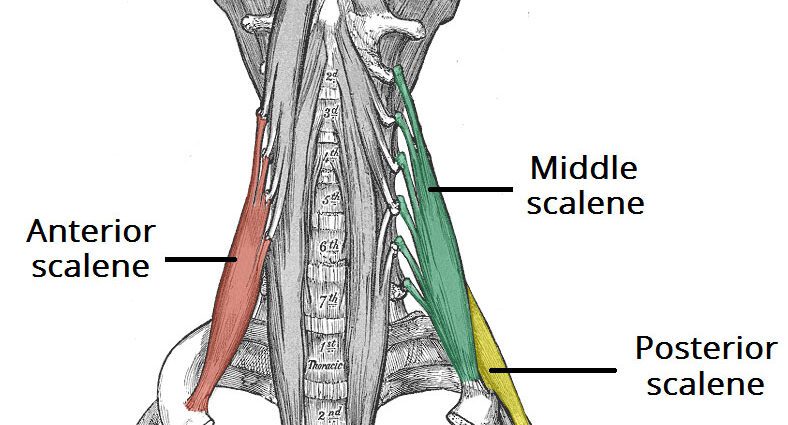
There are, in fact, three bundles of scalene muscles:
- an anterior scalene muscle;
- a middle scalene muscle;
- a posterior scalene muscle.
These scalene muscles are stretched between the cervical processes, that is, the bony protrusions of the cervical vertebrae located on the spine, and the first two pairs of ribs. These muscles are distributed bilaterally, in front and to the side.
Physiology of scalene muscles
The physiological and biomechanical function of scalene muscles is to be flexor muscles. These three muscles make it possible to move the neck sideways. In addition, certain muscles of the neck and the shoulder girdle are also involved in breathing: this is the case of the scalene muscles, which contribute to inspiration during calm breathing.
In bilateral contraction, the scalene muscles are flexors of the cervical spine and inspirers. In unilateral contraction, they are ipsilateral tilters and rotators.
Abnormalities / pathologies of scalene muscles
The main anomalies or pathologies linked to the scalene muscle are constituted by the scalene syndrome. This syndrome reflects the compression of the vascular and nervous bundle, during its passage between the anterior and middle scalene muscles.
The causes of such compression can be of several orders:
- poor posture, such as drooping shoulders or keeping the head forward;
- trauma, for example caused by a car accident, an anatomical defect (cervical rib);
- pressure on the joints, which can be caused by obesity or by carrying an oversized bag or backpack that can put excessive pressure on the joints;
- muscular hypertrophy linked to the practice of certain sports;
- or pregnancy, which can lead to sagging joints.
The treatment of scalene syndrome as well as its progression need to be adapted to each patient. It may seem surprising that such a small muscle can cause so many clinical signs. In fact, the main treatment will be essentially physiotherapy type.
It will require great precision as well as great rigor during processing. Many physiotherapy exercises can be offered, to which are also added other exercises such as active or passive mobilizations, or massage therapy techniques, that is to say, literally, “a massage that heals”.
Against the spasm, breathing work is essential because it will relax these muscles. Eight times out of ten, rehabilitation therapy is effective and sufficient to relieve pain in patients.
What diagnosis?
The diagnosis of scalene syndrome is difficult to make, since there are no pathognomonic signs. It is, therefore, one of the most complex entities in medicine, from a pathogenetic, diagnostic and therapeutic point of view. In fact, the diagnosis will be medical but also physiotherapeutic. Indeed, this physiotherapeutic diagnosis will follow the medical diagnosis, which will have made it possible to determine the competence of the physiotherapist to treat the patient and to rule out all etiologies other than cervicarthrosis.
This scalene syndrome is also called thoraco-brachial crossing syndrome (STTB) or thoraco-brachial outlet syndrome (TBDS). It can be expressed in many ways, which is why its diagnosis is so difficult to make: the clinical signs are varied, they can be vascular and / or neurological. In addition, they lack specificity.
Regarding neurological forms, women are twice as affected as men, between 30 and 50 years old. As for venous forms, they are twice as frequent in the male population, according to the figures given by Doctor Hervé de Labareyre, sports doctor in Paris.
History of the description of scalene syndrome
The first true clinical case of STTB described is due to the British surgeon Sir Ashley Cooper in 1821, with a good description of the symptoms by Mayo in 1835. The “Thoracic Outlet syndrome” was first described in 1956 by Peet. Mercier named it in 1973 Thoraco-brachial crossing syndrome.
It should be noted that the scalene syndrome, or STTB, represents a global concept bringing together the problems of compression of the neurological and vascular elements of the hilum of the upper limb. And it is in particular in view of the importance of the common physiopathological factor represented by the compression of the first rib that Roos proposes, in 1966, its resection by the transaxillary route. Peet, from the Mayo Clinic, offers a rehabilitation protocol.
Concretely, it is the work of Mercier and his collaborators that has revived the interest in the question in France.