









Contents
Diaphragmatic hernia
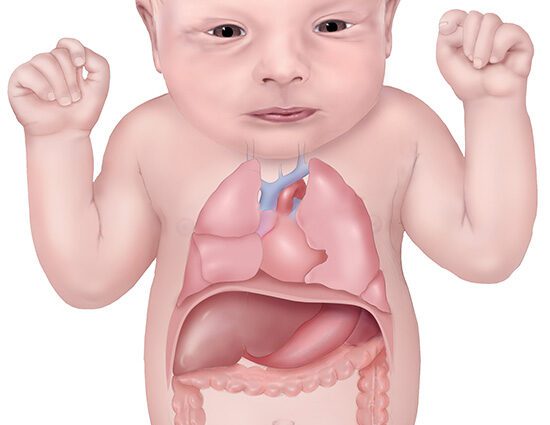
Diaphragmatic hernia is a rare and severe condition of congenital or traumatic origin. It results from the formation of a breach in the muscle of the diaphragm, through which the viscera from the abdominal cavity ascend into the chest cavity and compress the lungs. After surgical treatment, significant sequelae may remain.
What is a diaphragmatic hernia?
Definition
A hernia is the removal of an organ, total or partial, from its usual location.
In diaphragmatic hernias, a defect in the diaphragm allows the organs of the abdomen to ascend into the chest cavity.
Congenital diaphragmatic hernia (HDC) results from incomplete formation of the diaphragm during embryonic development. The intrusion of the abdominal viscera into the chest cavity compromises the development of the lungs.
There are several varieties of HDC:
- Bochdalek’s hernia (80-92% of cases) usually forms at the back and side of the diaphragm, on the left in most cases. The kidney, spleen, pancreas, liver, small intestine or colon are likely to move up into the chest. Cardiac, digestive, neurological or urogenital malformations are associated in 10 to 50% of cases.
- Much less common, Morgagni’s hernia is also often more favorable. The breach in the diaphragm is behind the breastbone, usually on the right side, with bilateral hernias being much rarer.
Post-traumatic diaphragmatic hernia occurs in adults when the diaphragm ruptures following severe trauma.
Hiatus hernia can be considered a diaphragmatic hernia. In this much more benign and widespread condition, a portion of the stomach moves up into the mediastinum (between the two lungs) through a small opening called the esophageal hiatus.
Causes
Congenital diaphragmatic hernia
The origin of congenital diaphragmatic hernia is not known. It appears as a result of an error in the placement of the various components of the diaphragm during development. In particular, Bochdalek’s hernia appears between the ninth and tenth week of pregnancy due to a failure to close an opening called the pleuropenitoneal duct.
Post-traumatic diaphragmatic hernia
Road accidents are responsible for nine out of ten post-traumatic diaphragmatic hernias. Knife or firearm injuries can also be involved.
Diagnostic
- Congenital diaphragmatic hernia
Bochdalek’s hernia is often detected during the 2nd mandatory ultrasound. The diagnosis is confirmed by a reference ultrasound performed in a multidisciplinary prenatal diagnosis center (CPDPN). In particular, it makes it possible to measure lung volume and to visualize the position of the liver and other organs liable to be herniated. Deviation of the heart and excess amniotic fluid (hydramnios) are often observed.
Additional examinations are then performed:
- Amniocentesis is suggested to perform a karyotype (study of chromosomal abnormalities).
- Fetal cardiac ultrasound is used to study the morphology of the heart.
- MRI provides a somewhat more accurate measurement of lung volume than ultrasound.
In the absence of an antenatal diagnosis, the doctor may be alerted at birth by respiratory distress, a bulging and immobile chest on the side of the hernia, a hollowed out abdomen, deviated heart sounds …
In 11% of cases, Bochdalek’s hernia goes unnoticed and will be discovered by chance many years later. Morgagni’s hernia is often discovered by chance in elderly children or adults.
- Post-traumatic diaphragmatic hernia
A chest x-ray allows the diagnosis a little more than half of the time. The scanner is the reference examination to establish a complete assessment of the lesions. However, the diagnosis is not always easy because the imaging does not visualize the rupture of the diaphragm.
Persons concerned
- Congenital diaphragmatic hernia
HDC concerns around 1/3500 births, or 350 babies per year.
In 40% of cases, other malformations are associated with it, linked in some cases to chromosomal and genetic abnormalities. The prognosis is all the more gloomy as these malformations are severe. HDC appears in particular in fetuses with trisomy 18 or 13 or with Fryns, Denys-Drash or Pallister-Killian syndrome.
- Congenital diaphragmatic hernia
Diaphragm ruptures occur in approximately 5% of severe multiple trauma, and more rarely in trauma patients hospitalized for thoracic and / or abdominal contusion.
Symptoms of diaphragmatic hernias
Congenital diaphragmatic hernia
The wide variety of possible symptoms reflects the association to varying degrees of several functional and anatomical abnormalities.
The ascent of the abdominal viscera into the thoracic cavity causes:
- insufficient development of the lungs (pulmonary hypoplasia)
- pulmonary arterial hypertension (PAH),
- insufficient development of the left ventricle of the heart in major forms, when the hernia is located on the left side.
Although the prognosis is generally severe (survival rate of children born alive from 30 to
60%), the course of the disease is much more favorable if the diaphragm closure abnormality appears late during gestation and if the orifice is small. The symptoms depend on the extent of the hernia and the nature of the herniated organs.
In adults, Bochdalek’s hernia can cause:
- chest pain
- difficulty in breathing
- abdominal pain
- digestive disorders.
In Morgagni’s hernia, the symptoms are less present and less specific.
Complications
Half of living children are prone to complications:
- chronic pulmonary arterial hypertension (PAH),
- repeated viral infections,
- nutritional and digestive disorders, in particular gastroesophageal reflux,
- scoliosis or chest deformities,
- neurological disorders.
Post-traumatic diaphragmatic hernia
The clinical manifestations of a post-traumatic diaphragmatic hernia are very heterogeneous and can appear years after the accident.
The most frequent symptoms are mainly respiratory (shortness of breath, chronic cough, repeated respiratory infections, etc.) or digestive (nausea, vomiting, abdominal pain after meals, etc.).
Complications
Strangulation of the herniated viscera in the thorax is a major risk. It first manifests as a strong pain, and can very quickly lead to necrosis of the strangled viscus. It is therefore a medical and surgical emergency.
Management of diaphragmatic hernias
Congenital diaphragmatic hernia
Antenatal surgery
Still experimental, prenatal surgeries can be tried in some severe forms of HDC. This type of intervention consists of placing a balloon, or “plug”, in the trachea of the fetus. in utero around the 28th week of pregnancy. It aims to allow the lungs to grow better. The ball is withdrawn during the third half of the year.
The technique used (fetoscopic intervention combined with ultrasound) avoids having to open the uterus.
Neonatal care and surgery
At birth, babies with a severe form have great difficulty adjusting to extrauterine life. Childbirth is generally scheduled in such a way as to be able to plan for the intervention of resuscitation and neonatal teams. The management is heavy, with immediate intubation to allow the infant to breathe. Doctors then decide on the strategy to put in place to stabilize the child’s vital parameters before operating.
The surgical treatment of the hernia aims to put the abdominal viscera back in their place and to close the communication between the thorax and the abdomen.
Follow-up
The high risk of complications requires the establishment of specialized multidisciplinary follow-up from the neonatal period, and throughout childhood.
Returning home is not always easy and daily care by liberal professionals (nurses, physiotherapists, etc.) may remain necessary.
Nutritional disorders and digestive disorders can persist for several years. Oral disorders, which result in eating difficulties, must be taken care of by specially trained speech therapists.
Children also remain fragile on the pulmonary level, especially the first year, and rigorous hygiene measures must be observed to limit the risk of infection.
The growth of the child is carefully monitored, which should make it possible to detect and treat neurological disorders, scoliosis, etc. as soon as they appear.
Post-traumatic diaphragmatic hernia
surgery
Surgical treatment is required to avoid strangulation of the hernia. If sutures are not sufficient, a patch may be considered.
Mere baby nu pregnesi vich hrniya ho gyian Dr raminder narang kotkpoora hospital jis ne Sanu dasseya nhi mera baby ajj buht Sirius h 4 din da babby mooh ch sah len vali pipe lagai gyi abi tk Sirius h doctor da kehna 20%chance h