









Contents
Obstructed labor: what is shoulder dystocia?
During the expulsion, it may happen that the baby’s shoulders get stuck in the mother’s pelvis even though his head is already out. A rare but serious complication of childbirth, this dystocia is a vital emergency requiring a very precise obstetric maneuver to disengage the newborn without risk.
What is obstructed labor?
Greek dys meaning difficulty and tokos, delivery, obstructed delivery is what is commonly referred to as difficult delivery, as opposed to eutocic delivery, that is, one that takes place in accordance with the physiological process.
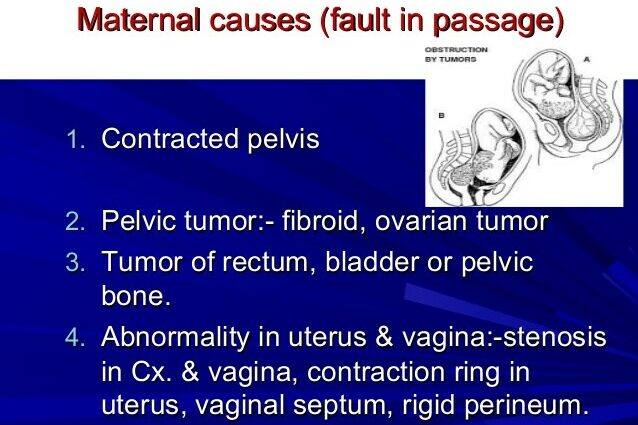
There are two main types of dystocia: maternal dystocia (abnormal uterine contractions, problems with the cervix, placenta previa, pelvis deformed or too small …) and dystocia of fetal origin (too large fetus, irregular presentation, shoulder dystocia). These various problems may require resorting to artificial rupture of membranes, the installation of an oxytocin infusion, the use of instruments (forceps, suction cups), episiotomy, cesarean section, etc.
The two types of shoulder dystocia
- The false dystocia. Also called “shoulder difficulty”, it concerns between 4 and 5 deliveries in 1000. Poorly positioned, the baby’s posterior shoulder hits the pubic symphysis.
- The real dystocia. More serious, it concerns between 1 childbirth in 4000 and 1 childbirth in 5000 and is characterized by a total absence of engagement of the shoulders in the pelvis.
How to cure shoulder dystocia?
Since the baby’s head is already out, it is not possible to deliver it by cesarean section. No question of pulling on his head or pressing violently on the mother’s uterus to release it very quickly. These actions could have dramatic consequences. To get him out very quickly without risk, the medical team has at its disposal several types of obstetric maneuvers, the choice of which will be made according to the situation. Here are the most popular:
- Mac Roberts’ maneuver is performed in case of false shoulder dystocia. The mother is lying on her back, her thighs bent towards her stomach and her buttocks at the edge of the delivery table. This hyperflexion makes it possible to enlarge the perimeter of the pelvis and to promote the rotation of the head to unblock the anterior shoulder. 8 times out of 10, this maneuver is enough to unblock the situation.
- Jacquemier’s maneuver is used in the event of true dystocia of the shoulders or in the event of failure of the maneuver of Mac Roberts. Much more intrusive, this technique consists, after having performed a large episiotomy on the side of the fetal back, in introducing a hand into the mother’s vagina in order to grab the baby’s hand corresponding to his posterior shoulder to lower the arm and thus free the other shoulder.
Risk factors for shoulder dystocia
If the occurrence of true shoulder dystocia is a very difficult event to predict during childbirth, doctors have nonetheless identified several risk factors: fetal macrosomia, i.e. a thinking baby. ultimately more than 4 kg; an overrun; excessive weight gain during pregnancy …
Complications of shoulder dystocia
Shoulder dystocia exposes the newborn to a risk of fracture of the collarbone and more rarely of the humerus, but also of obstetric paralysis of the brachial plexus. There are over 1000 cases of paralysis each year due to damage to the nerves of the brachial plexus. Three quarters recover with rehabilitation but the last quarter must undergo surgery. Fortunately, fetal deaths from asphyxia attributable to shoulder dystocia have become very rare (4 to 12 out of 1000 proven shoulder dystocia).
Shoulder dystocia can also be the cause of maternal complications, in particular cervico-vaginal tears, bleeding during delivery, infections, etc.