









Infectious spondylodiscitis: definition and treatment
Spondylodiscitis is a severe infection of one or more vertebrae and adjacent intervertebral discs. It is one of the many causes of back and spine pain. Uncommon, this condition represents 2 to 7% of osteoarticular infections. In some cases, spondylodiscitis causes compression in the spinal cord due to an abscess. This can reach and destroy nerve roots. It is therefore essential to treat this pathology urgently to avoid long-term complications. The management includes immobilization by bed rest and / or immobilization orthosis, and appropriate antibiotic therapy.
What is infectious spondylodiscitis?
The term spondylodiscitis comes from the Greek words spondulos which means vertebra and diskos which means disk. It is an inflammatory disease of one or more vertebrae and adjacent intervertebral discs.
Infectious spondylodiscitis is an uncommon condition. It represents 2 to 7% of osteomyelitis, that is to say osteoarticular infections. It concerns 1 cases per year in France, preferably men. If the average age of onset is around 200 years, 60% of patients are under 50 years, spondylodiscitis mainly affecting adolescents. During these two periods of life, the changes in the bones are more important, causing a greater vulnerability to the risk of infection. It is a serious disease presenting risks of spinal deformities and neurological sequelae.
What are the causes of infectious spondylodiscitis?
Contamination often occurs through the blood following sepsis. The germs involved are most often the following bacteria:
- pyogens, such as Staphylococcus aureus (bacteria identified in 30 to 40% of cases), Gram-negative bacilli such asEscherichia coli (20 to 30% of cases) and Streptococcus (10% of cases);
- Mycobacterium tuberculosis (in this case we speak of Pott’s disease);
- Salmonella;
- Brucelles.
More rarely, the germ can be a fungus such as candida albicans
While tuberculosis is found mainly in the thoracic region, infectious pyogenic spondylodiscitis affects:
- the lumbar spine (60 to 70% of cases);
- the thoracic spine (23 to 35% of cases);
- the cervical spine (5 to 15%);
- several floors (9% of cases).
Infectious spondylodiscitis can result from:
- a urinary, dental, skin (wound, whitlow, boil), prostate, cardiac (endocarditis), digestive or pulmonary infection;
- spinal surgery;
- a lumbar puncture;
- a minimally invasive local procedure for diagnostic (discography) or therapeutic (epidural infiltration).
Depending on the germ, two evolutionary modes can be distinguished:
- an acute course in case of pyogenic bacteria;
- a chronic course in cases of tuberculosis or pyogenic infections treated by insufficient antibiotic therapy.
The main risk factor is the alteration of the patient’s immune status. In addition, more than 30% of patients suffer from diabetes, around 10% from chronic alcoholism and almost 5% have one of the following pathologies:
- cancer;
- hepatic cirrhosis;
- end-stage renal disease;
- systemic disease.
What are the symptoms of infectious spondylodiscitis?
Infectious spondylodiscitis is one of the many causes of back pain, which is deep pain in the back and spine. They can be associated with:
- severe spinal stiffness;
- painful nerve irradiations: sciatica, cervicobrachial neuralgia;
- fever (in more than two-thirds of cases of pyogenic spondylodiscitis) and chills;
- weakening and compression of the vertebrae;
- a deterioration of the general condition.
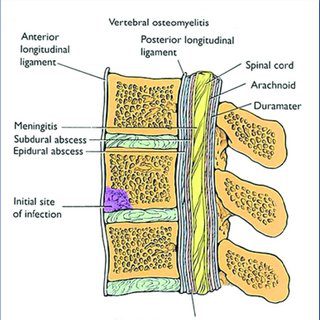
In some cases, infectious spondylodiscitis can cause infection of the meninges or compression of the spinal cord due to an abscess. This can reach and destroy nerve roots.
Depending on the importance of the infection and the type of bacteria, later consequences may occur such as a vertebral block, that is to say the welding of two opposite vertebrae.
How to treat infectious spondylodiscitis?
Infectious spondylodiscitis is a therapeutic emergency requiring hospitalization. Support includes:
Immobilization in bed
- a cast shell or a corset can help calm severe pain and prevent deformity resulting from vertebral compression, especially in the case of Pott’s disease;
- until the pain has ceased in the case of pyogenic spondylodiscitis (10 to 30 days);
- for 1 to 3 months in the case of Pott’s disease.
Long-lasting intense antibiotic therapy adapted to the germ
- for staphylococcal infections: combination cefotaxime 100 mg / kg and fosfomycin 200 mg / kg then combination fluoroquinolone – rifampicin;
- for infections of hospital origin resistant to methicillin: combination vancomycin – fucidic acid or fosfomycin;
- For gram-negative bacilli infections: combination of 3rd generation cephalosporin and fosfomycin, 3rd generation cephalosporin and aminoglycoside or fluoroquinolone and aminoglycoside;
- In the event of Pott’s disease: quadruple anti-tuberculosis antibiotic therapy for 3 months then bichimotherapy for the following 9 months.
Surgery in exceptional cases
- decompressive laminectomy in cases of sudden spinal cord compression;
- evacuation of an epidural abscess.
The course is usually favorable. Fever and spontaneous pain usually go away within 5 to 10 days. Mechanical pain under load disappears within 3 months.