









Contents
What is hip dysplasia
Hip dysplasia is the congenital immaturity of the bones, tendons, and ligaments at the junction of the femoral head and acetabulum that form the joint. In simple words – incomplete development of the joint.
In the risk group for the disease are mainly children born with a large weight and in the breech presentation.
The diagnosis does not need to be frightened, “the child will not walk” or “will limp all his life” – this is possible only with an extreme form of hip dysplasia. In most cases, children with hip dysplasia walk normally, but in violation of the “docking” of the femoral head and the cavity of the hip joint, the load is distributed unevenly as the child grows and his activity increases and can lead to complications.
It is important to identify the disease in time in childhood to prevent premature violation of the hip joint in adolescence and adulthood.
Causes of hip dysplasia in children
There are several factors that can affect the appearance of hip dysplasia in a child:
- heredity. This pathology is more often observed in children whose father and mother suffered from congenital developmental disorders of the hip joint;
- severe toxicosis;
- taking any medication during pregnancy;
- large fruit;
- gluteal presentation;
- lack of water;
- gynecological problems.
Symptoms of hip dysplasia in children
- instability of the hip joint;
- displacement and return to its original position of the femoral head;
- limited abduction of the affected hip joint;
- asymmetrical folds on the back of the thighs;
- obvious shortening of the affected leg.
The very first sign that can be seen in a newborn is hip instability, but in 80% of all cases this goes away on its own.
Treatment of hip dysplasia in children
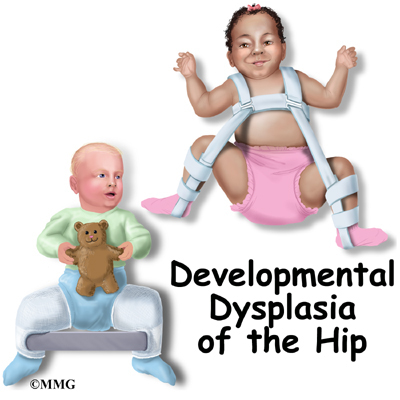
Treatment of dysplasia includes a fixed position with the help of soft orthopedic devices that spread the legs (Freik’s pillow, Pavlik’s stirrups, Becker’s panties, Vilensky’s or Volkov’s elastic splints) and therapeutic exercises.
Diagnostics
– If your child is suspected of hip dysplasia, it is necessary to conduct an ultrasound of the hip joints and / or X-ray examination, – says Mikhail Mashkin.
The most difficult thing to diagnose is hip dysplasia of the 1st degree (pre-luxation). In this case, only the asymmetry of the skin folds and a positive symptom of a click can be detected (a characteristic click is heard, indicating the reduction of the dislocation when the legs are bent at the knee and hip joints to the sides).
Hip dysplasia of the 2nd degree (subluxation) in infants is diagnosed by identifying asymmetric skin folds, a positive click symptom, and a symptom of limited hip abduction.
With hip dysplasia of the 3rd degree (dislocation), the disease is pronounced, that the parents of the child can notice the violations. Studies are needed to fully confirm the diagnosis.
If there are signs of hip dysplasia in a child, an ultrasound examination is prescribed in 100% of cases. X-ray is the most informative diagnostic method, starting from the seventh month of life.
Therapies
Modern conservative treatment of hip dysplasia in children is based on the following basic principles: giving the limb an ideal position for reduction (flexion and abduction), the earliest possible start, maintaining active movements, long-term continuous therapy, the use of additional methods of exposure (therapeutic exercises, massage, physiotherapy).
Conservative treatment involves long-term therapy under the control of ultrasound and X-ray examination.
The most common method of treating hip dysplasia is wide swaddling for up to 3 months, Freik pillow or Pavlik stirrups until the end of the first half of the year, and in the future – various abduction splints for aftercare of residual defects.
For children with hip dysplasia, physiotherapy exercises (exercise therapy) are indicated from the first days of life. It ensures the full physical and mental development of the child.
Also, from the first days of a child’s life with a pathology, massage is prescribed – it helps prevent secondary muscle dystrophy, improves blood circulation in the affected limb and thus contributes to the speedy elimination of the pathology.
Operations are indicated only with a rough structure of the joint, when conservative treatment will be ineffective. Surgical methods are also used when the reduction of dislocation without surgery is impossible.
Prevention of hip dysplasia in children at home
- do biochemical and ultrasound screenings during pregnancy on time;
- do not swaddle the child tightly, do not straighten the legs when swaddling;
- if there is a reception with a foot, do not use jumpers;
- the child must wear shoes with a solid back;
- taking vitamin D3 (to begin with, consult a pediatrician);
- preventive examinations of the child by an orthopedist at 1, 3, 6 months and 1 year after he learns to walk.
Popular questions and answers
Answers Mikhail Mashkin, PhD, certified osteopath, chiropractor, orthopedist.