









Contents
In line with its mission, the Editorial Board of MedTvoiLokony makes every effort to provide reliable medical content supported by the latest scientific knowledge. The additional flag “Checked Content” indicates that the article has been reviewed by or written directly by a physician. This two-step verification: a medical journalist and a doctor allows us to provide the highest quality content in line with current medical knowledge.
Our commitment in this area has been appreciated, among others, by by the Association of Journalists for Health, which awarded the Editorial Board of MedTvoiLokony with the honorary title of the Great Educator.
A neonatal haemolytic disease is a condition caused by an incompatibility (conflict) in Rh factor or AB0 blood groups between mother and fetus. The ailment causes the production of antibodies in the mother’s blood, which in turn leads to the breakdown of the red blood cells of the fetus and the newborn. The most dangerous form of hemolytic disease is jaundice.
A few words about the hemolytic disease of the newborn …
The ailment is related to a serological conflict, i.e. a situation in which the mother’s blood group is different from the child’s blood group. Haemolytic disease causes the production of antibodies in the mother’s blood which breaks down the red blood cells of the fetus and newborn. The most dangerous form of the disease is severe neonatal jaundice, caused by rapidly increasing levels of bilirubin in the blood and the development of anemia. When the bilirubin level exceeds a certain threshold, it can damage the brain, known as jaundice of the testicles of the base of the brainwhich results – if the child survives – psychophysical underdevelopment. Currently, the serological conflict is not as big a problem as in the XNUMXth century.
The causes of the hemolytic disease of the newborn
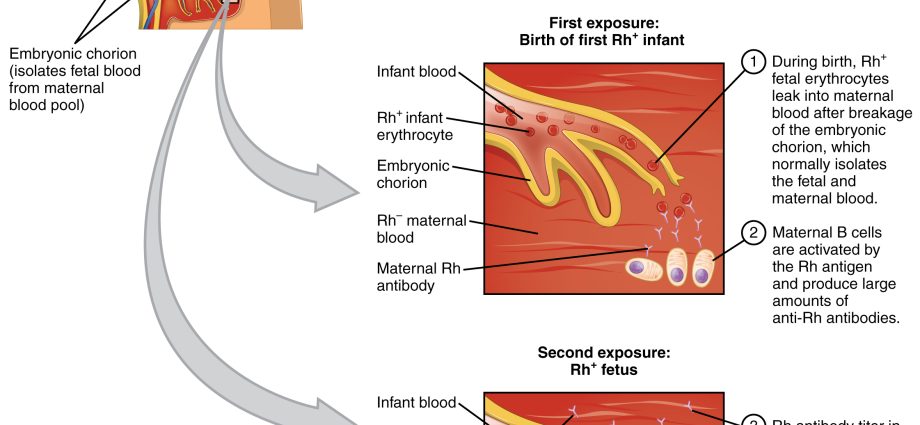
Everyone has a specific blood group, and under normal conditions a healthy body does not produce antibodies against its blood cells. The Rh + blood group does not produce antibodies against this factor, i.e. anti-Rh. Similarly, the body of a patient with blood group A does not produce anti-A antibodies. However, this rule does not apply to pregnant women, therefore the hemolytic disease of the newborn is caused by a conflict between the baby’s blood and the antibodies produced by the mother. To put it simply: the mother’s blood is allergic to the baby’s blood. A pregnant woman’s antibodies can cross the placenta (in the present or next pregnancy) and attack the baby’s blood cells. The consequence is then the haemolytic disease of the child.
Symptoms and forms of a child’s hemolytic disease
The mildest form of haemolytic disease is the excessive destruction of the baby’s blood cells. A child is born with anemiausually accompanied by an enlarged spleen and liver, but this does not pose a threat to his life. Over time, the blood picture improves significantly and the baby develops properly. However, it should be emphasized that in some cases anemia is severe and requires specialist treatment.
Another form of hemolytic disease there is severe jaundice. Your baby appears to be completely healthy, but begins to develop jaundice on the first day after birth. There is a very rapid increase in bilirubin, which is responsible for the yellow color of the skin. Jaundice is a great danger because its concentration beyond a certain level has a toxic effect on the baby’s brain. It can even lead to brain damage. In children with jaundice, seizures and excessive muscle tension are observed. Even if a child is saved, jaundice can have serious consequences, for example, a child may lose his hearing, suffer from epilepsy and even have difficulty speaking and maintaining balance.
The last and most serious form of hemolytic disease of the newborn is generalized fetal swelling. As a result of the destruction of the baby’s blood cells by the mother’s antibodies (still at the stage of fetal life), the circulation of the newborn is disturbed and the permeability of its vessels is increased. What does it mean? The fluid from the blood vessels escapes to adjacent tissues, thus causing internal edema to form in important organs, such as the peritoneum or the pericardial sac that surrounds the heart. At the same time, the toddler develops anemia. Unfortunately, fetal swelling is so serious that it most often leads to fetal death while still in the womb or right after birth.
Diagnostics of the haemolytic disease of the newborn
Typically, a pregnant woman will undergo screening tests to identify the presence of anti-RhD or other equally relevant antibodies. Usually, in the first trimester of pregnancy, the antiglobulin test (Coombs test) is performed if the child’s parents are RhD incompatible. Even if the result is negative, the test is repeated every trimester and one month before delivery. In turn, a positive test result is an indication for extending the diagnosis and performing tests of the type and titer of antibodies. Low antibody titer (below 16) requires only conservative treatment, i.e. monthly monitoring of the antibody titer. On the other hand, the diagnosis of high antibody titers (over 32) requires more invasive treatment. An indication for this is also the identification of the umbilical vein dilatation, hepatomegaly and thickened placenta on ultrasound. Then, aminopuncture and cordocentesis (obtaining a fetal blood sample for testing) are performed. These tests allow to accurately assess how advanced the fetal anemia is, to assess the blood type and the presence of appropriate antigens on the blood cells. Normalized results require the test to be repeated after a few weeks.
Treatment is initiated when severe anemia is found. Moreover, a PCR method is performed which confirms the presence of the D antigen. The lack of this antigen excludes the occurrence of haemolytic disease of the fetus.
Hemolytic disease of the newborn – treatment
Treatment of ailments mainly involves intrauterine exogenous blood transfusion under ultrasound guidance. The blood is given into the vascular bed or into the peritoneal cavity of the fetus. 3-4 transfusion cycles are required for complete blood exchange. Therapy should be continued until the fetus is capable of ectopic life. In addition, doctors recommend ending pregnancy to a maximum of 37 weeks. After birth, the newborn often requires albumin transfusions and phototherapy, in more severe cases, replacement or complementary transfusion is performed. In addition to treatment, disease prevention is also important.
Hemolytic disease of the newborn – prophylaxis
Haemolytic disease prophylaxis may be specific and non-specific. The first is to avoid contact with foreign blood and to follow the rules of group compatible blood transfusion after cross-matching. The second, in turn, is based on the application of anti-D immunoglobulin 72 hours before the expected blood leak, that is:
- during childbirth,
- in the event of a miscarriage,
- in case of bleeding during pregnancy,
- as a result of invasive procedures performed during pregnancy,
- during ectopic pregnancy surgery.
As intra-pregnancy prophylaxis in Rh negative women with negative antiglobulin test results, the administration of anti-D immunoglobulins (at the 28th week of pregnancy) is used. The next dose of immunoglobulins is given only after the baby is born. This method only secures for one, closest pregnancy. In women who are planning even more children, immunoprophylaxis is used once again.