









Contents
Anisocytosis is a term for a blood abnormality. We speak of anisocytosis when there is a difference in size between several blood cells of the same cell line, such as red blood cells (erythrocyte anisocytosis) and platelets (platelet anisocytosis).
What is anisocytosis
Anisocytosis is a term used in hematology when there is a size abnormality between blood cells of the same cell line such as:
- red blood cells, also called red blood cells or erythrocytes;
- blood platelets, also called thrombocytes.
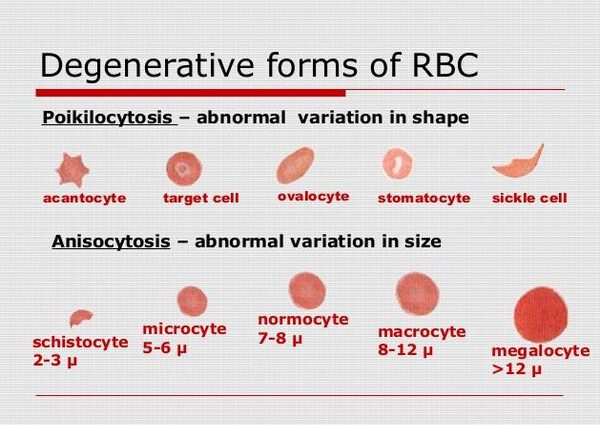
Anisocytosis is a laboratory phenomenon characterized by the presence of abnormally sized erythrocytes (less than 6 microns or greater than 8 microns) in the peripheral blood. This condition can be observed with iron deficiency anemia, vitamin deficiency, bleeding, etc. Anisocytosis is diagnosed by morphological examination of a blood smear, as well as by a high red blood cell distribution width index (RDW). Elimination of anisocytosis is carried out as part of the treatment of the underlying disease.
What are the different types of anisocytosis?
It is possible to distinguish several anisocytoses depending on the cell line concerned:
- erythrocyte anisocytosis when the abnormality concerns erythrocytes (red blood cells);
- platelet anisocytosis, sometimes called thrombocytic anisocytosis, when the abnormality concerns the thrombocytes (blood platelets).
Depending on the type of abnormality found, anisocytosis is sometimes defined as:
- anisocytosis, more often abbreviated as microcytosis, when the blood cells are abnormally small;
- aniso-macrocytosis, more often abbreviated as macrocytosis, when the blood cells are abnormally large.
How to detect anisocytosis?
Anisocytosis is a blood abnormality identified during a hemogram, also called Blood Count and Formula (NFS). Carried out by taking a sample of venous blood, this examination provides a great deal of data on blood cells.
Among the values obtained during a blood count, the red blood cell distribution index (RDI) is also called the anisocytosis index. Making it possible to assess the variability in the size of red blood cells in the bloodstream, this index makes it possible to identify erythrocyte anisocytosis. It is considered normal when it is between 11 and 15%.
What are the causes of anisocytosis?
Generally speaking, anisocytosis is a term used by doctors to refer to erythrocyte anisocytosis. With regard to red blood cells, this blood abnormality is usually due to anemia, an abnormal drop in the level of red blood cells or hemoglobin in the blood. This deficiency can cause complications because red blood cells are cells essential for the distribution of oxygen within the body. Present in red blood cells, hemoglobin is a protein capable of binding several molecules of oxygen (O2) and releasing them in cells.
It is possible to distinguish several types of anemia causing erythrocyte anisocytosis, including:
- theiron deficiency anemia, caused by iron deficiency, which is considered microcytic anemia because it can lead to anisocytosis with the formation of small red blood cells;
- vitamin deficiency anemia, the most common of which are vitamin B12 deficiency anemias and vitamin B9 deficiency anemias, which are considered macrocytic anemias because they can cause aniso-macrocytosis with the production of large deformed red blood cells.
- thehemolytic anemia, characterized by premature destruction of red blood cells, which can be caused by genetic abnormalities or diseases.
Platelet anisocytosis also has a pathological origin. Platelet anisocytosis can in particular be due to myelodysplastic syndromes (MDS), which constitute a set of diseases due to dysfunction of the bone marrow.
Specific Causes of anisocytosis
Physiological
Not always the presence of anisocytosis indicates any pathology. For example, in newborns, physiological macrocytosis is observed. This is due to the gradual maturation of the bone marrow and the processes of mitosis in hematopoietic stem cells. By the 2nd month of life, anisocytosis slowly resolves on its own.
iron deficiency
The most common pathological cause of anisocytosis is iron deficiency. With a lack of iron in the body, there is a violation of the maturation of erythrocytes, the formation of their cell membrane, and the formation of hemoglobin. As a result, the size of red blood cells decreases (microcytosis). With a pronounced lack of iron, the total content of hemoglobin in the blood decreases, and iron deficiency anemia (IDA) develops.
Together with anisocytosis, hypochromia very often occurs, i.e. reduced hemoglobin saturation of erythrocytes. Anisocytosis, along with other changes in erythrocyte indices (MCV, MCH, MCHC), may precede the development of IDA, in the so-called latent iron deficiency.
Also, anisocytosis may persist at the start of iron supplementation for the treatment of iron deficiency anemia. Moreover, it has a rather specific character – there are a large number of both microcytes and macrocytes in the blood, which is why the histogram of the distribution of erythrocytes has a characteristic two-peak appearance.
Causes of iron deficiency:
- Alimentary factor.
- Childhood, adolescence, pregnancy (periods of increased need for iron).
- Profuse prolonged menstruation.
- Chronic blood loss: peptic ulcer of the stomach or duodenum, hemorrhoids, hemorrhagic diathesis .
- Condition after resection of the stomach or intestines.
- Genetic disorders of iron metabolism: hereditary atransferrinemia.

Vitamin B12 and folic acid deficiency
Another cause of anisocytosis, namely macrocytosis, is B12 deficiency with folic acid, and a joint vitamin deficiency is very often observed . This is due to their closely occurring metabolic reactions. The lack of B12 prevents the transition of folic acid into an active, coenzyme form. This biochemical phenomenon is called the folate trap.
The lack of these vitamins leads to a violation of purine and pyrimidine bases (the main components of DNA), which primarily affects the work of the bone marrow, as an organ with the highest activity of cell proliferation. A megaloblastic type of hematopoiesis arises – not fully matured cells with elements of the cell nucleus, increased saturation of hemoglobin and increased size enter the peripheral blood, i.e. anemia is macrocytic and hyperchromic in nature.
The main causes of B12 deficiency:
- Strict diet and exclusion of animal products.
- atrophic gastritis.
- Autoimmune gastritis.
- Resection of the stomach.
- Hereditary deficiency of intrinsic factor Castle.
- Malabsorption : celiac disease, inflammatory bowel disease.
- Worm infestations: diphyllobothriasis .
- Genetic defect of transcobalamin.
However, isolated folate deficiency may occur. In such cases, the only pathological change in the blood may be anisocytosis (macrocytosis). This is mainly found in alcoholism, as ethyl alcohol slows down the absorption of folate in the gastrointestinal tract. Also, a lack of folic acid and subsequent macrocytosis occurs in patients who take oral contraceptives for a long time, in pregnant women.
Thalassemia
In some cases, anisocytosis (microcytosis), along with hypochromia, may be signs of thalassemia, a group of diseases characterized by a genetic abnormality in the synthesis of globin chains. Depending on the mutation of a particular gene, there is a lack of some globin chains and an excess of others (alpha, beta or gamma chains). Due to the presence of defective hemoglobin molecules, red blood cells decrease in size (microcytosis), and their membrane is more susceptible to destruction (hemolysis).
Hereditary microspherocytosis
In Minkowski-Choffard disease, due to a mutation of the gene encoding the formation of structural proteins of the erythrocyte membrane, the permeability of their cell wall increases in red blood cells, and water accumulates in them. Erythrocytes decrease in size and become spherical (microspherocytes). Anisocytosis in this disease is often combined with poikilocytosis.
Sideroblastic anemias
Very rarely, anisocytosis may be due to the presence of sideroblastic anemia, a pathological condition in which the utilization of iron is impaired, while the iron content in the body may be normal or even elevated. Causes of sideroblastic anemia:
- Myelodysplastic syndrome (most common cause).
- Taking medications that disrupt the metabolism of vitamin B6.
- Chronic lead intoxication.
- Mutation of the ALAS2 gene.
Diagnostics
The detection of the conclusion “anisocytosis” in the form of a blood test requires an appeal to a general practitioner to determine the cause of this condition. At the appointment, the doctor collects a detailed history, reveals the presence of complaints characteristic of anemia (general weakness, dizziness, deterioration in concentration, etc.). Clarifies whether the patient is taking any medications on an ongoing basis.
During an objective examination, attention is drawn to the presence of clinical symptoms of anemic syndrome: pallor of the skin and mucous membranes, low blood pressure, increased heart rate, etc. For hereditary hemolytic anemia, the presence of signs of deformation of the bone skeleton is characteristic.
Additional studies are scheduled:
- General blood analysis. In the KLA, the indicator of the hematological analyzer, reflecting the presence of anisocytosis, is RDW. However, it may be erroneously high due to the presence of cold agglutinins. Therefore, a microscopic examination of a blood smear is mandatory. Also, microscopy can detect signs of B12 deficiency (Jolly bodies, Kebot rings, hypersegmentation of neutrophils) and other pathological inclusions (basophilic granularity, Pappenheimer bodies).
- Blood chemistry. In a biochemical blood test, the level of serum iron, ferritin, and transferrin is checked. Markers of hemolysis may also be noted – an increase in the concentration of lactate dehydrogenase and indirect bilirubin.
- Immunological research. If an autoimmune lesion of the gastrointestinal tract is suspected, tests are performed for antibodies to the parietal cells of the stomach, antibodies to transglutaminase, and gliadin.
- Detection of abnormal hemoglobin. In the diagnosis of thalassemia, hemoglobin electrophoresis on cellulose acetate film or high performance liquid chromatography is performed.
- Diagnosis of microspherocytosis. To confirm or exclude hereditary microspherocytosis, the osmotic resistance of erythrocytes and the EMA test are carried out using the fluorescent dye eosin-5-maleimide.
- parasitological research. In case of suspicion of diphyllobothriasis, microscopy of a native fecal preparation is prescribed to search for eggs of a wide tapeworm.
Sometimes it is required to conduct a differential diagnosis between IDA and thalassemia minor. This can be done already by a general blood test. For this, the Mentzer index is calculated. The ratio of the MCV to the number of red blood cells more than 13 is typical for IDA, less than 13 – for thalassemia.

What are the symptoms of anisocytosis?
The symptoms of anisocytosis are those of anemia. Although there are different forms and origins of anemia, several characteristic symptoms are frequently observed:
- a feeling of general fatigue;
- shortness of breath
- palpitations;
- weakness and dizziness;
- pallor;
- headaches.

How to treat anisocytosis?
Treatment for anisocytosis depends on the cause of the abnormality. In the event of iron deficiency anemia or vitamin deficiency anemia, nutritional supplementation may for example be recommended to treat anisocytosis.
Treatment of anisocytosis
Conservative therapy
There is no isolated correction of anisocytosis. To eliminate it, treatment of the underlying disease is necessary. When deficiencies of vitamins and microelements are detected, the first stage of therapy is the appointment of a diet with the inclusion of foods rich in iron, vitamin B12 and folic acid. The following treatments are also available:
- Pharmacological correction of iron deficiency. Iron preparations are used to treat IDA and latent iron deficiency. Preference is given to ferrous iron, as it has a higher bioavailability. However, if the patient has peptic ulcer, preparations containing ferric iron are recommended, since they are less irritating to the gastrointestinal mucosa.
- Vitamin therapy. Vitamin B12 is prescribed in injectable form. An increase in the number of reticulocytes on the 7-10th day from the start of the drug administration indicates the effectiveness of the treatment. Folic acid is taken in tablet form.
- Fight against hemolysis. Glucocorticosteroids and intravenous immunoglobulin are used to stop hemolysis . Hydroxyurea is used to prevent hemolytic crises.
- Deworming. To eliminate a wide tapeworm, specific chemotherapy drugs are used – derivatives of pyrazinisoquinoline, which cause spastic contraction of the muscles of helminths, which leads to their paralysis and death.
- Blood transfusions . The basis of the treatment of thalassemia, hereditary microspherocytosis is regular transfusions of whole blood or erythrocyte mass, which depends on the severity of anemia.
Surgery
The ineffectiveness of conservative therapy for Minkowski-Chauffard disease or thalassemia is an indication for the complete removal of the spleen – total splenectomy . Preparation for this operation must necessarily include vaccination against pneumococcus , meningococcus and Haemophilus influenzae. In rare cases of diphyllobothriasis, with the development of intestinal obstruction, surgery (laparoscopy, laparotomy) is performed, followed by the extraction of a wide tapeworm.
Literature 1. Anemia (clinic, diagnosis, treatment) / Stuklov N. I., Alpidovsky V. K., Ogurtsov P. P. – 2013. 2. Anemia (from A to Z). Guidelines for doctors / Novik A.A., Bogdanov A.N. – 2004. 3. Differential diagnosis of anemia not associated with iron metabolism / N.A. Andreichev // Russian medical journal. – 2016. – T.22(5). 4. Iron deficiency states and iron deficiency anemia / N.A. Andreichev, L.V. Baleeva // Bulletin of modern clinical medicine. – 2009. – V.2. – AT 3. |
super explicație, mulțumesc!