









Vitamin B12 deficiency anemia
This form of anemia occurs as a result of a lack of vitamin B12 (cobalamin). Vitamin B12 is essential for the formation of red blood cells, in particular. This anemia forms very slowly, after months or years of vitamin deficiency. The elderly are the most affected: about 12% of them are said to be suffering from a deficiency in this vitamin, without there necessarily being anemia1.
Vitamin B12 is obtained by consuming foodstuffs of animal origin, such as meat, eggs, fish and shellfish. For most people, food gives the body much more B12 than it needs. The excess is stored in the liver. It is possible to suffer from anemia from a lack of B12 in the diet, but it is rare. Most often, anemia results from a problem withabsorption of vitamins.
THEpernicious anemia would affect 2% to 4% of the general population2. It is most likely underdiagnosed because the symptoms are not always obvious to detect.
Causes
An inability to do well absorber vitamin B12 contained in food: this cause is the most common. Here are the main elements that can lead to poor absorption.
- A lack of intrinsic factor. Intrinsic factor is a molecule secreted in the stomach which allows the absorption of vitamin B12 in the small intestine by binding to it (see diagram). For the binding between intrinsic factor and B12 to occur, there must be a normal degree of acidity in the stomach. When anemia is caused by a lack of intrinsic factor, it is calledpernicious anemia or Biermer’s anemia. Genetic factors would intervene.
- Low acidity in the stomach. 60% to 70% of vitamin B12 deficiencies in elderly would be due to a lack of gastric acidity1. With age, stomach cells secrete less stomach acid and also less intrinsic factor. Regular and prolonged intake of pharmaceuticals antacids3, such as histamine blockers (eg ranitidine) but particularly from the class of proton pump inhibitors (eg omeprazole), also increase the risk1.
- Taking metformin. People who take metformin, most often to treat diabetes, are at greater risk for vitamin B12 deficiency4.
- Autoimmune disease (Graves’ disease, thyroiditis, vitiligo, etc.): in these cases, autoantibodies will bind the intrinsic factor, making it unavailable to bind vitamin B12.
- Chronic bowel disease, which prevents the passage of vitamin B12 through the intestinal wall (for example, Crohn’s disease, ulcerative colitis, or celiac disease). Taking vitamin supplements is usually suggested by the doctor to prevent deficiencies. In the case of celiac disease, absorption of vitamin B12 returns to normal once the gluten-free diet is adopted. Any other disease leading to malabsorption, such as chronic pancreatitis or very rarely parasite infestation can cause vitamin B12 deficiency.
- Certain stomach or small intestine surgeries. Patients receive preventive vitamin B12 supplementation.
Anemia may also be due to a lack of vitamin B12 in supply. But this situation is rather rare, since it only takes small amounts of B12 to meet the body’s needs. In addition, this one has the capacity to make important reserves, which can be sufficient to the needs during 3 or 4 years. Adherents of strict vegetarianism (also called veganism), which do not consume protein of animal origin, can suffer from anemia, in the long term, if they do not otherwise meet their B12 needs (see Prevention). Research has shown that 92% of vegans are deficient in vitamin B12 if they do not take a supplement, compared to 11% of omnivores.5.
Evolution
THEvitamin B12 deficiency anemia sets in very slowly, insidiously. However, this anemia can be treated quickly and easily. From the first days of treatment, the symptoms subside. Within a few weeks, the deficiency can usually be corrected.
However, it is important to treat this type of anemia, because over the years, neurological symptoms may appear (numbness and tingling in the extremities, gait disturbance, mood swings, depression, psychosis, symptoms of dementia, etc.). These symptoms take longer to disappear (sometimes 6 months or more). Sometimes there are still sequelae.
People with pernicious anemia are also slightly more at risk of stomach tumors than the rest of the population.
Diagnostic
THEanemia caused by B12 deficiency can be detected by various blood tests. The following abnormalities are signs:
- a decrease in the number of red blood cells, white blood cells and platelets;
- a decrease in the hematocrit, that is to say the volume occupied by red blood cells relative to that of blood;
- a lowered hemoglobin level;
- an increased size of red blood cells (mean globular volume or MCV): it may however remain stable if iron deficiency anemia (iron deficiency) is also present;
- a change in the appearance of red blood cells and white blood cells, which can be seen by examining a blood smear.
- There can be vitamin B12 deficiency without anemia.
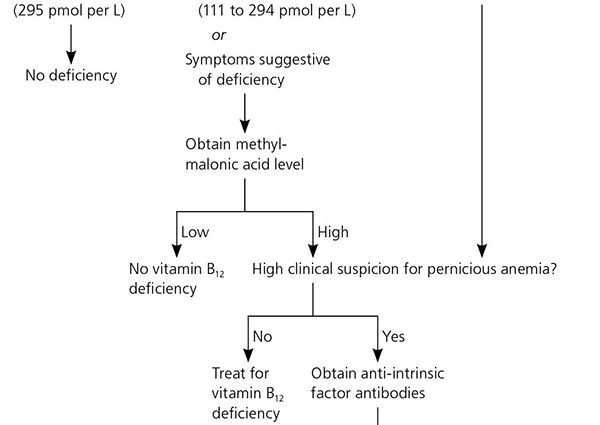
The doctor also checks the levels of vitamin B12, folic acid and iron in the blood. We must also find out the cause of the anemia. If vitamin B12 deficiency is detected, testing for intrinsic factor autoantibodies is often undertaken.
Remark. The deficiency of folic acid (vitamin B9) produces the same type of effect on the red blood cells: they enlarge and become deformed. However, B9 deficiency anemia does not cause neurological symptoms. |