









Contents
Treacher-Collins syndrome
A rare genetic disease, Teacher-Collins syndrome is characterized by the development of birth defects of the skull and face during embryonic life, resulting in deformities of the face, ears and eyes. The aesthetic and functional consequences are more or less severe and some cases require numerous surgical interventions. However, in most cases, taking charge allows a certain quality of life to be preserved.
What is Treacher-Collins Syndrome?
Definition
Treacher-Collins syndrome (named after Edward Treacher Collins, who first described it in 1900) is a rare congenital disease that manifests itself from birth with more or less severe malformations of the lower part of the body. face, eyes and ears. The attacks are bilateral and symmetrical.
This syndrome is also called Franceschetti-Klein syndrome or mandibulo-facial dysostosis without end abnormalities.
Causes
Three genes have so far been known to be involved in this syndrome:
- the TCOF1 gene, located on chromosome 5,
- the POLR1C and POLR1D genes, located on chromosomes 6 and 13 respectively.
These genes direct the production of proteins that play a key role in the embryonic development of facial structures. Their alteration through mutations disrupts the development of bone structures (mainly those of the lower and upper jaws and cheekbones) and soft tissues (muscles and skin) of the lower part of the face during the second month of gestation. The pinna, the ear canal as well as the structures of the middle ear (ossicles and / or eardrums) are also affected.
Diagnostic
Facial malformations can be suspected from the ultrasound of the second trimester of pregnancy, especially in cases of significant ear malformations. In this case, the prenatal diagnosis will be established by a multidisciplinary team from magnetic resonance imaging (MRI) of the fetus, allowing the malformations to be visualized with more precision.
Most of the time, the diagnosis is made by a physical examination done at birth or soon after. Due to the great variability of malformations, it must be confirmed in a specialized center. A genetic test on a blood sample may be ordered to look for the genetic abnormalities involved.
Some mild forms go unnoticed or will be detected fortuitously late, for example following the appearance of a new case in the family.
Once the diagnosis is made, the child is subjected to a series of additional examinations:
- facial imaging (x-ray, CT scan and MRI),
- ear exams and hearing tests,
- vision assessment,
- search for sleep apnea (polysomnography) …
The people concerned
Treacher-Collins syndrome is thought to affect one in 50 newborns, both girls and boys. It is estimated that around 000 new cases appear each year in France.
Risk factors
Genetic counseling in a referral center is recommended to assess the risks of genetic transmission.
About 60% of cases appear in isolation: the child is the first patient in the family. Malformations occur following a genetic accident that affected one or other of the reproductive cells involved in fertilization (“de novo” mutation). The mutated gene will then be passed on to his descendants, but there is no particular risk for his siblings. However, it should be checked whether one of his parents is not actually suffering from a minor form of the syndrome and carrying the mutation without knowing it.
In other cases, the disease is hereditary. Most often, the risk of transmission is one in two with each pregnancy, but depending on the mutations involved, there are other modes of transmission.
Symptoms of Treacher-Collins syndrome
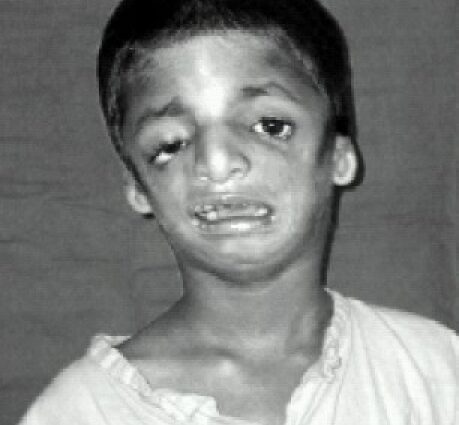
The facial features of those affected are often characteristic, with an atrophied and receding chin, non-existent cheekbones, eyes tilted downwards towards the temples, ears with small and badly hemmed pavilion, or even completely absent …
The main symptoms are linked to malformations of the ENT sphere:
Respiratory difficulties
Many children are born with narrow upper airways and narrowly open mouths, with a small oral cavity largely obstructed by the tongue. Hence significant breathing difficulties especially in newborns and infants, which are expressed by snoring, sleep apnea and too weak breathing.
Difficulty eating
In infants, breastfeeding may be hampered by difficulty in breathing and by abnormalities of the palate and soft palate, sometimes split. Feeding is easier after the introduction of solid foods, but chewing can be difficult and dental problems are common.
Deafness
Hearing discomfort due to malformations of the outer or middle ear is present in 30 to 50% of cases.
Visual disturbances
One third of children suffer from strabismus. Some may also be nearsighted, hyperopic or astigmatic.
Learning and communication difficulties
Treacher-Collins syndrome does not cause intellectual deficit, but deafness, visual problems, speech difficulties, the psychological repercussions of the disease as well as the disturbances induced by often very heavy medical care can cause a delay. language and difficulty communicating.
Treatments for Treacher-Collins syndrome
Infant care
Breathing support and / or tube feeding may be necessary to facilitate breathing and feeding the infant, sometimes from birth. When respiratory assistance must be maintained over time, a tracheotomy (small opening in the trachea, at the neck) is performed to introduce a cannula directly ensuring the passage of air in the airways.
Surgical treatment of malformations
More or less complex and numerous surgical interventions, relating to the soft palate, jaws, chin, ears, eyelids and nose can be proposed to facilitate eating, breathing or hearing, but also to reduce the aesthetic impact of malformations.
As an indication, the slits of the soft palate are closed before the age of 6 months, the first cosmetic procedures on the eyelids and cheekbones from 2 years, the lengthening of the mandible (mandibular distraction) towards 6 or 7 years old, reattachment of the ear pinna at around 8 years old, enlargement of the auditory canals and / or surgery of the ossicles around 10 to 12 years old… Other cosmetic surgery operations can still be performed at the adolescence…
Hearing aid
Hearing aids are sometimes possible from the age of 3 or 4 months when deafness affects both ears. Different types of prostheses are available depending on the nature of the damage, with good efficiency.
Medical and paramedical follow-up
In order to limit and prevent disability, regular monitoring is multidisciplinary and calls on various specialists:
- ENT (high risk of infection)
- Ophthalmologist (correction of visual disturbances) and orthoptist (eye rehabilitation)
- Dentist and orthodontist
- Speech Therapist…
Psychological and educational support is often necessary.