









Contents
Tako Tsubo syndrome or broken heart syndrome
Tako Tsubo syndrome is a disease of the heart muscle characterized by transient dysfunction of the left ventricle. Since its first description in Japan in 1990, Tako Tsubo syndrome has gained worldwide recognition. However, after 30 years of considerable effort to better understand this disease, current knowledge remains limited.
Definition of broken heart syndrome
Tako Tsubo syndrome is a disease of the heart muscle characterized by transient dysfunction of the left ventricle.
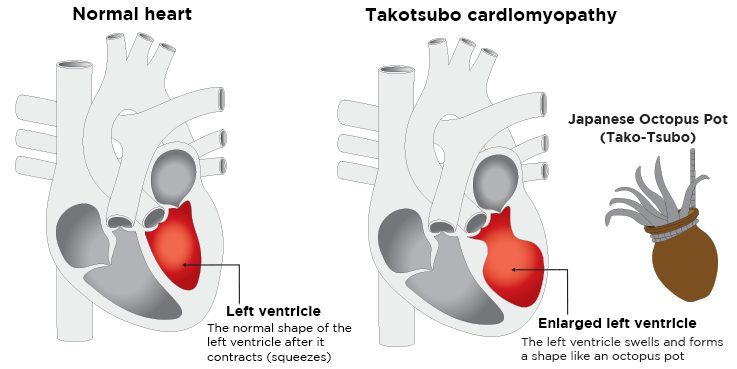
This cardiomyopathy takes its name from the Japanese “octopus trap”, due to the shape the left ventricle takes in most cases: bloating at the top of the heart and narrowing at its base. Takotsubo syndrome is also known as “broken heart syndrome” and “apical ballooning syndrome”.
Who is concerned ?
Takotsubo syndrome accounts for about 1 to 3% of all patients worldwide. According to the literature, about 90% of patients with the syndrome are women aged between 67 and 70 years. Women over 55 have a five times higher risk of developing the disease than women under 55 and ten times higher risk than men.
Symptoms of Tako Tsubo syndrome
The most common symptoms of Tako Tsubo syndrome are:
- Sharp chest pain;
- Dyspnea: difficulty or difficulty in breathing;
- A syncope: sudden loss of consciousness.
The clinical manifestation of Takotsubo syndrome induced by severe physical stress may be dominated by the manifestation of the underlying acute disease. In patients with ischemic stroke or seizure, Takotsubo syndrome is less often accompanied by chest pain. In contrast, patients with emotional stressors have a higher prevalence of chest pain and palpitations.
It is important to note that a subset of patients with Takotsubo syndrome may present with symptoms arising from its complications:
- Heart failure;
- Pulmonary edema;
- A cerebral vascular accident ;
- Cardiogenic shock: failure of the heart pump;
- Cardiac arrest ;
Diagnostic du syndrome de Takotsubo
The diagnosis of Takotsubo syndrome is often difficult to distinguish from acute myocardial infarction. However, in some patients it can be diagnosed incidentally through changes in the electrocardiogram (ECG) or a sudden rise in cardiac biomarkers – products released into the blood when the heart is damaged.
Coronary angiography with left ventriculography – qualitative and quantitative radiography of left ventricular function – is considered the gold standard diagnostic tool to rule out or confirm the disease.
A tool, called an InterTAK score, can also quickly guide a diagnosis of Takotsubo syndrome. Rated out of 100 points, the InterTAK score is based on seven parameters:
- The female sex (25 points);
- The existence of psychological stress (24 points);
- The existence of physical stress (13 points);
- The absence of depression of the ST segment on the electrocardiogram (12 points);
- Psychiatric history (11 points);
- Neurological history (9 points);
- Prolongation of the QT interval on the electrocardiogram (6 points).
A score greater than 70 is associated with a probability of the disease equal to 90%.
Causes of broken heart syndrome
Most Takotsubo syndromes are triggered by stressful events. Physical triggers are more common than emotional stressors. On the other hand, male patients are more often affected by a physical stressful event, while in women an emotional trigger is more frequently observed. Finally, cases also occur in the absence of an obvious stressor.
Physical triggers
Among the physical triggers are:
- Physical activities: intensive gardening or sport;
- Different medical conditions or accidental situations: acute respiratory failure (asthma, end-stage chronic obstructive pulmonary disease), pancreatitis, cholecystitis (inflammation of the gallbladder), pneumothorax, traumatic injuries, sepsis, chemotherapy, radiotherapy, pregnancy, cesarean section, lightning, near-drowning, hypothermia, cocaine, alcohol or opioid withdrawal, carbon monoxide poisoning, etc.
- Certain medications, including dobutamine stress tests, electrophysiological tests (isoproterenol or epinephrine), and beta-agonists for asthma or chronic obstructive pulmonary disease;
- Acute obstruction of the coronary arteries;
- Affections of the nervous system: stroke, head trauma, intracerebral hemorrhage or convulsions;
Psychological triggers
Among the psychological triggers are:
- Grief: the death of a family member, friend or pet;
- Interpersonal conflicts: divorce or family separation;
- Fear and panic: theft, assault or public speaking;
- Anger: an argument with a family member or landlord;
- Anxiety: personal illness, childcare or homelessness;
- Financial or professional problems: gambling losses, business bankruptcy or job loss;
- Others: lawsuits, infidelity, incarceration of a family member, loss in legal action, etc. ;
- Natural disasters such as earthquakes and floods.
Finally, it should be noted that the emotional triggers of the syndrome are not always negative: positive emotional events can also cause the disease: a surprise birthday party, the fact of winning a jackpot and a positive job interview, etc. This entity has been described as “happy heart syndrome”.
Treatments for Takotsubo syndrome
After a first case of Takotsubo syndrome, patients are at risk of recurrence, even years after. Certain substances seem to show an improvement in survival at one year and a decrease in this recurrence rate:
- ACE inhibitors: they inhibit the conversion of angiotensin I to angiotensin II – an enzyme that causes blood vessels to constrict – and increase the levels of bradykinin, an enzyme with vasodilating effects;
- Angiotensin II receptor antagonists (ARA II): they block the action of the eponymous enzyme.
- An antiplatelet drug (APA) may be considered on a case-by-case basis after hospitalization in the event of severe left ventricular dysfunction associated with persistent apical bloating.
The potential role of excess catecholamines – organic compounds synthesized from tyrosine and acting as a hormone or neurotransmitter, the most common of which are adrenaline, norepinephrine and dopamine – in the development of Takotsubo cardiomyopathy has been debated for a long time, and as such, beta blockers have been proposed as a therapeutic strategy. However, they do not seem to be effective in the long term: a recurrence rate of 30% is observed in patients treated with beta-blockers.
Other therapeutic avenues remain to be explored, such as anticoagulants, hormonal treatments for menopause or psychotherapeutic treatment.
Risk factors
The risk factors for Takotsubo syndrome can be classified into three main types:
- Hormonal factors: the striking preponderance of postmenopausal women suggests a hormonal influence. Lower estrogen levels after menopause potentially increase women’s susceptibility to Takotsubo syndrome, but systematic data demonstrating a clear link between the two is lacking so far;
- Genetic factors: it is possible that a genetic predisposition can interact with environmental factors to favor the onset of the disease, but here too, studies allowing this assertion to be generalized are lacking;
- Psychiatric and Neurological Disorders: A high prevalence of psychiatric – anxiety, depression, inhibition – and neurological disorders has been reported in patients with Takotsubo syndrome.