









Contents
Prevention and medical treatment of thyroid nodule
Prevention
– Iodine deficiency should be avoided, as it is a risk factor for thyroid nodules.
– Radiation treatments are better and better adapted so as to deliver only the minimum dose necessary in each case, and limit the impact on the thyroid.
The diagnosis
The doctor first determines, with the help of various examinations, the nature of the nodule. Treatment or no treatment is chosen accordingly. Before the 1980s, the majority of nodules were removed by surgery. Since then, diagnostic and treatment methods have been refined in order to operate only when essential.
L’exam clinique
Examination of the neck will confirm or not that the swelling is linked to the thyroid, check whether it is painful or not, single or multiple, hard, firm or soft, and look for the presence of lymph nodes in the neck
The general exam looks for signs of abnormal thyroid function
The doctor will also ask what treatments are usually taken by the person, the notion of a history of thyroid problems in the family, irradiation of the neck in childhood, the geographical origin, the contributing factors (tobacco, lack of iodine, pregnancy)
Thyroid hormone assay
The blood test of the hormone TSH regulating the production of thyroid hormones makes it possible to check whether the secretion of thyroid hormones is normal, excessive (hyperthyroidism) or insufficient (hypothyroidism) .The dosage of thyroid hormones T3 and T4 is only required if the TSH is abnormal. We also look for the presence of anti-thyroid antibodies. Calcitonin is requested if a particular form of cancer is suspected, medullary thyroid cancer.
Ultrasound
This is the preferred method for diagnosing thyroid nodules. It makes it possible to visualize nodules of 2 mm in diameter or more and to know the number of nodules and the possible presence of multinodular goiter. Imaging is also used to differentiate the solid, liquid or mixed appearance of the nodule. Depending on its appearance and its size it gives arguments in favor of the benign or malignant character which lead to ask or not a puncture. It also allows after the treatment to follow the evolution of the nodule.
Thyroid scan
It is only requested when the TSH hormone dosage is low.
To do a thyroid scintigraphy, after taking radioactive markers such as iodine or technetium, we observe the way in which iodine is distributed in the thyroid gland.
This examination specifies the overall functioning of the gland, may show nodules not seen on palpation and looks for whether the nodules are “cold” it is with decreased thyroid hyperfunction, “hot” with excessive production of hormones, or “neutral »With normal hormonal functioning.
A hot nodule is almost always benign, so it is not a priori cancer. Cold nodules are cancer a bit more often, although 90% are still mild.
The puncture of a nodule under ultrasound control is requested if the clinical characteristics or the appearance on ultrasound suggest the malignant nature of the nodule. (cf. sheet) Using a fine needle, the doctor aspirates the cells of the nodule for a microscopic examination of their characteristics and to assess the nature, benign or cancerous, of the nodule. It also helps to evacuate a cystic nodule.
The puncture will be renewed if it is inconclusive
These examinations can be supplemented by a thyroid scintigraphy, a CT scan or an MRI. When thyroid cancer is suspected, it is often the surgical intervention with histological examination of the tumor which makes it possible or not to confirm it.
Treatments
Radioactive iodine. It is often used as an adjunct to thyroid cancer surgery to destroy any thyroid cells that may not have been removed by surgery.
Radioactive iodine is also used to treat (“hot”) nodules causing symptoms of hyperthyroidism. A treatment of 2 to 3 months is normally enough for the nodules to resolve and for the symptoms of hyperthyroidism to disappear. Iodine is taken orally in capsule or liquid form. This treatment causes permanent hypothyroidism in about 80% of cases, because the radioactive iodine destroys the cells that produce the hormones. This hypothyroidism secondary to treatment can be well compensated by treatment with thyroid hormones then taken regularly. In some cases, the nodules are treated with surgery.
surgery. It removes one lobe or the entire thyroid (thyroidectomy). It is indicated when the nodules are cancerous or suspected of malignancy, or if they are hypersecreting (making too much thyroid hormone) or large. Lifelong thyroid hormone replacement therapy (levothyroxine) is most often required. Thereafter, the operated person will therefore take replacement thyroid hormones every day.
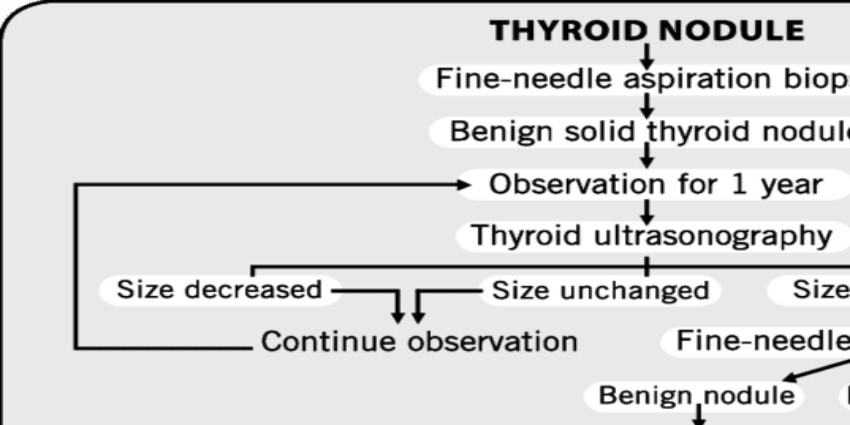
Nodules without hormonal secretion disorders and whose volume is less than ¾ cm are monitored every 6 months to a year.