









Contents
Pregnancy hemorrhoids
What is a hemorrhoid?
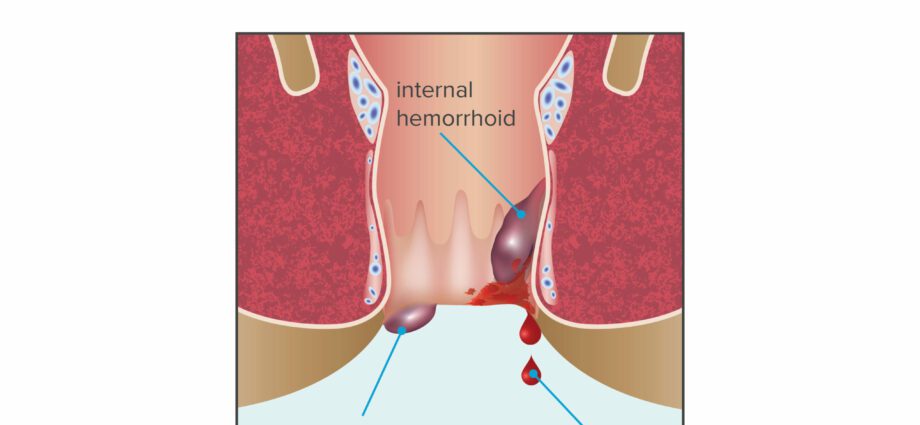
Hemorrhoids are small vascular pads located in the submucosa of the anal canal (internal hemorrhoids) and directly under the skin at the margin of the anus (external hemorrhoids). These are completely normal anatomical entities that play an important role in anal continence. But sometimes congestion, inflammation or thrombosis occurs in one or more of these hemorrhoids. We can then distinguish different pathologies:
- hemorrhoidal crisis: it results in a sensation of heat or gravity perineal, accentuated in the saddle. It usually lasts 2 to 4 days.
- Hemorrhoidal thrombosis: due to the formation of a small clot in an internal or external hemorrhoid, it results in severe pain and can lead to bleeding in the stool.
- hemorrhoidal prolapse: the internal hemorrhoid appears during defecation, or even permanently, causing severe discomfort and pain.
Risk factors during pregnancy
During pregnancy, various factors will promote the occurrence of hemorrhoids, especially during the third trimester:
- -modification of venous return, itself induced by the increase in blood volume, hormonal impregnation which causes relaxation of tissues including venous, and the gravid uterus which compresses the pelvic region.
- -constipation (via efforts to defecate) due to a decrease in intestinal motility, itself a consequence of hormonal changes and the weight of the uterus.
- – a relaxation of the tissues under the effect of hormones, knowing that the hemorrhoidal tissue is very rich in estrogenic receptors and therefore very sensitive to hormonal variations (2).
The intense expulsion efforts during childbirth also promote the appearance of hemorrhoids after childbirth.
Multiple management of pregnancy hemorrhoids
During pregnancy, the management of hemorrhoids is based on hygiene and dietetic rules and drug treatments.
- it is advisable to carry out a local toilet after each bowel movement with a neutral soap, a lotion or washing foam based on burdock. In the event of associated pruritus, it is recommended to use instead of toilet paper a cotton wool soaked in a toilet milk based on sweet almond oil (3
- it is essential to fight against constipation by starting by adopting the classic hygienic-dietetic measures, namely good hydration and a sufficient fiber intake (fruits and vegetables, whole grains). If constipation persists, laxatives can be used knowing that during pregnancy, laxatives of ballast based on mucilage (sterculia, ispaghul, psyllium, guar or bran gum), osmotic laxatives (macrogol, lactulose, lactitol, sorbitol) are preferred. ), and if necessary occasionally, a lubricating laxative (4).
- local treatment: a cream containing a local anesthetic with or without corticosteroids may be prescribed during pregnancy (5).
- to relieve the pain, it is possible to take an analgesic. Paracetamol is the gold standard analgesic throughout pregnancy, but in the event of severe hemorrhoidal pain, more powerful analgesics containing morphine derivatives may be prescribed during pregnancy (6).
- in the event of associated venous insufficiency, oral venotonic treatment may be prescribed. Diosmin, hesperidin, troxerutin and rutoside are the preferred molecules (7) in pregnant women.
Instrumental treatments (sclerosing injections, infrared photocoagulation, rubber bands, cryotherapy, mono and bipolar coagulation) and surgery should be avoided during pregnancy (8).