









Contents
Menstrual cycle: the luteal phase
The last phase of the menstrual cycle, the luteal phase plays a key role in female fertility by allowing, in the event of fertilization, the implantation of the egg and the maintenance of the pregnancy. How is it going? When should it be supported? Some elements of explanation.
The luteal phase in the ovarian cycle: the last phase of the cycle
The menstrual cycle is divided into several phases, essential for the production of the oocyte and the maintenance of pregnancy after fertilization:
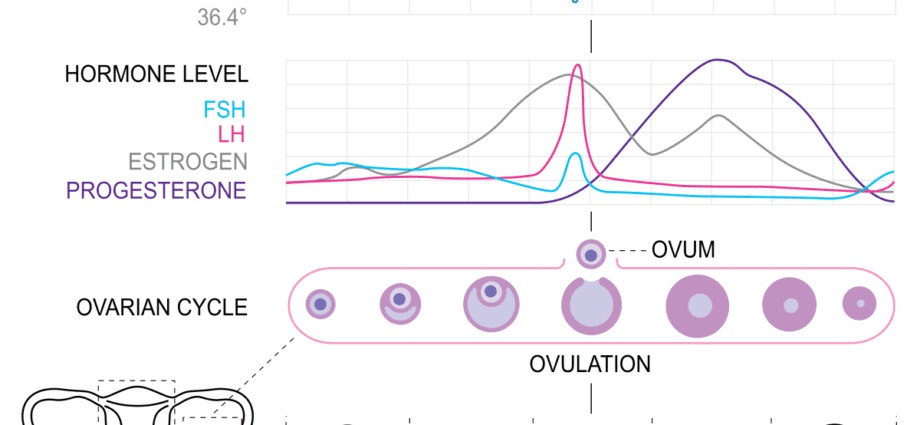
- the follicular phase lasts about 14 days from the first day of your last period. During this phase, several oocytes enveloped in their ovarian follicle, a cell that resembles a small sac, begin to mature under the influence of pituitary hormone (FSH). Only one of them will be expelled.
- l’ovulation : During these 24 to 48 hours, which mark the middle of the ovarian cycle, the secretion of luteinizing hormone (LH) increases significantly. Its role: to cause the rupture of the follicle and the expulsion of the mature oocyte. This is called ovular laying or ovulation. In the hours following ovulation, the oocyte travels to the fallopian tube where it waits before being fertilized … or breaking down.
- luteal phase constitutes the last part of the ovarian cycle. This period between ovulation and the next period lasts between 12 and 14 days. During the luteal phase and under the effect of hormonal impregnation, the ovarian follicle is transformed into a gland which takes its name from its pigmentation: the yellow body. This corpus luteum is a key element in the prospect of a future pregnancy. Indeed, by secreting estrogen and progesterone, it prepares the lining of the uterus (endometrium) to receive the egg in the event of fertilization. It is for this reason that it thickens significantly during this second part of the cycle until the 20th day.
The luteal phase after fertilization … or not
After ovulation and therefore during the luteal phase, two scenarios are possible:
The oocyte is fertilized.
In this case, the embryo settles in the endometrium about 8 days after fertilization. It is implantation. Several hormones then play a key role:
- the hormone HCG, or chorionic gonadotropin, is secreted so that the corpus luteum continues its activity for 3 months. It is this hormone that is “screened” in the pregnancy test and allows you to know if you have fallen pregnant.
- estrogen and progesterone are secreted by the corpus luteum in order to maintain the pregnancy. This hormonal production persists for a few weeks until the placenta is ready to ensure gas and nutrient exchanges between mother and child.
The oocyte is not fertilized.
If there has been no fertilization, the oocyte does not nest in the endometrium and the corpus luteum no longer produces progesterone. With hormonal desimpregnation, the small vessels of the endometrium constrict and the mucous membrane breaks off causing hemorrhages. These are the rules. The follicular phase begins again.
Symptoms of the luteal phase
The most suggestive sign of the luteal phase is an increase in body temperature. This is because the production of progesterone by the corpus luteum causes the body to warm up by about 0,5 ° C. After a drop in temperature at the time of ovulation (the least “hot” moment of the cycle), body temperature remains around 37,5 ° C (on average) throughout this last phase of the cycle. menstrual.
Another more surprising characteristic of the luteal phase: the evolution of appetite. Indeed, hormonal production has, according to some studies, an influence on calorie intake during the cycle. Lower during the follicular phase, it would increase particularly in the pre-ovulatory phase and in the late luteal phase. In question: the impregnation in progesterone and estrogen, which would imply a decrease in the production of serotonin (the hormone of pleasure) and therefore a phenomenon of “food compensation” where women would favor carbohydrates, calcium and magnesium.
Infertility: the importance of supporting the luteal phase
The luteal phase is the subject of special observation in women who have difficulty getting pregnant or have suffered repeated miscarriages. The first-line solution is then to carry out a fertility check-up and to identify a possible ovulation disorder, in particular by observing the temperature curves and / or performing hormonal assays and a pelvic ultrasound.
If subfertility is suspected, ovarian stimulation may in some cases be recommended. It is within the framework of these techniques of aid to procreation (and more particularly IVF and IVF ICSII) that the support for the luteal phase is decisive. Indeed, by stimulating the ovaries to obtain as many eggs as possible (before in vitro fertilization), a malformation of the luteal phase is induced. The yellow bodies multiplied by the stimulation are then unable to produce enough progesterone, which can jeopardize the implantation of the embryo (s). Therefore, a treatment is put in place to promote the maintenance of the pregnancy. Two molecules are then favored:
- progesterone, usually administered vaginally,
- gonadotropin-releasing hormone (GnRH) agonists which stimulate the production of GnRH, a hormone that promotes the development of the corpus luteum.