









Contents
Hyperlipidemia (Cholesterol and triglycerides)
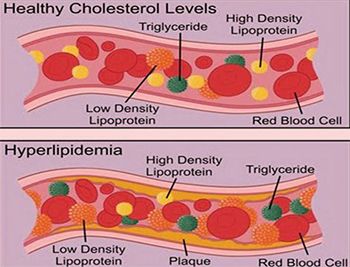
THEhyperlipidémia, it is the fact of having a high level of lipids in the blood (excess fat), which includes cholesterol and triglycerides. This physical condition does not cause symptoms. For many people, it has no negative consequences. Yet it is one of the most important of the many risk factors that, taken together, can lead to cardiovascular disease.
Excess lipids in the blood help to harden and thicken the lining of the arteries of the heart, coronary arteries. As a result, the heart adapts more and more with difficulty to physical exertion. Hyperlipidemia, by damaging the lining of the arteries, also contributes to the formation of blood clots which can completely block an artery causing a cerebrovascular accident (stroke), a heart attack (heart attack). Thickened plaques in the artery walls can also break off and get carried into the circulation (fat embolism) and then migrate to small arteries that they block, for example causing a stroke..
Objective: to avoid or delay disorders cardiovascular
The unrest cardiovascular are the leading cause of death on the planet1. In Canada, for example, cardiac disorders have become the second leading cause of death (28% of deaths), just behind cancer (29% of deaths)3.
Even though smoking has halved, the increase in overweight, obesity and also turn of waist (in the abdominal region) (approximately 5 cm to 6 cm more in the last 20 years50) portends an increased frequency of cardiovascular disorders for years to come.
However, it should be noted that these cardiovascular disorders are less often fatal than in the past: the death rate has fallen by around 40% in recent decades. For stroke, the management is also becoming more and more effective.
Where does excess cholesterol and triglycerides come from?
Le liver produces the vast majority of cholesterol (4 / 5th) used by the body in various functions. The rest comes fromfood, especially animal foods. It is foods high in saturated fat (fatty meats, butter, fatty dairy products) and trans fats (hydrogenated margarines, vegetable shortening, desserts, pastries) that raise the level of “bad” cholesterol, called LDL. However, we now know that for most people, dietary cholesterol alone has little effect on blood cholesterol levels: it only influences the blood cholesterol level for 1/5. Thus, eggs, shrimps and organ meats, for example, which are high in cholesterol, should not be banned, as they contain little saturated fat.
In addition to the food ingested, lack of physical activity (sedentary lifestyle) and smoking can also elevate cholesterol levels. Moreover, the Genoa have their influence in particular in large autosomal dominant familial hyperlipidemias.
Cholesterol is a specifically animal molecule, absent from plants. It allows the absorption of dietary fat through the formation of bile. Cholesterol also allows the production of hormones so it is essential for life, we cannot live without cholesterol.
As to triglycerides, they most often come from alcohol and sugars ingested excessively (especially “fast” sugars, such as fruit juices and other sugary drinks, cakes, confectionery and jams), converted into triglycerides by the liver. So even though triglycerides are a type of lipid (and therefore fat) in the blood, their excess presence does not usually come from dietary fat, but rather from excess sugars.
An expert’s point of view
Dr Martin Juneau, cardiologist Director of Prevention at the Montreal Heart Institute Do sugary foods have as big an impact as fatty foods on blood lipids? Fatty foods have the most negative effect on blood lipids, but sugary foods also influence them and play an equally important role as fatty foods in general health. Over the past 25 years, there has been a lot of accusation that fat is harmful to the arteries and the heart, but in the last 4 or 5 years or so, some very good research teams have realized that we have probably put too much fat on it. emphasis on fats and not enough on sugars. We have talked a lot about cholesterol, saturated fat, trans fat. The industry’s instinct has been to remove fat everywhere: low-fat yogurts, cholesterol-free products, etc. But to improve the taste, we tended to add sugar. Today, several experts believe that the obesity epidemic is attributable to this industry reaction. Nowadays, we eat more but especially we eat more sugar. We have certainly neglected the consequences of this excess sugar. Sugar influences blood lipids, especially through insulin metabolism. When you eat a sweet dessert, say a piece of cake or a sweet yogurt, your insulin goes up to lower blood sugar. When insulin is high in the blood, it causes a multitude of reactions. For example, a few hours after eating this dessert, your liver will start making more triglycerides. It also produces a little more LDL cholesterol, but the effect of sugar on this type of blood lipid is milder. And more generally, by raising the insulin level, sugar causes fat storage. The fats that lodge in the viscera increase the waistline and secrete a host of pro-inflammatory and oxidative substances. Inflammation is certainly linked to cardiovascular disease and possibly cancer as well. The point of view of Dr Cocaul Arnaud, nutritionist doctor in Paris Our Western diet is more a source of triglycerides than cholesterol. Thus per day, we ingest through food, about 120 g of triglycerides and 0,5 to 1 g of cholesterol Prevention obesity goes through intra-family nutritional education (knowing that education already begins for the child in the mother’s womb, hence the importance of the food choice of pregnant women). The explosion in sales of sugary drinks in France as elsewhere in the world among young people poses a real public health problem because it favors the surge in obesity figures.. We must educate our young people to drink water and not something else. The other thing must be punctual and reserved for festive occasions. Detecting hepatic steatosis (fatty liver) in young people is more and more frequent and suggests all the complications that will ensue because the obese young subject has time to age and therefore to deteriorate Parents’ concern should not be the fight against cholesterol, which remains a mysterious and disturbing word, but rather the fight against triglycerides, the level of which depends directly on the content of sucrose, fructose and other sugars in our daily diet.
|
How to detect hyperlipidemia?
By a lipid profile made from blood tests (the doctor writes on the prescription: explanation for lipid abnormality), we measure:
- the quantity of LDL cholesterol, or “bad cholesterol”;
- the quantity of triglycerides;
- the quantity of HDL cholesterol, or “good” cholesterol;
- the amount total cholesterol (CT).
Depending on the case, other blood tests may be offered by the doctor. For example, measuring the level of Lp (a) (lipoprotein a significantly elevated in people with simultaneously high LDL-C) and measuring C-reactive protein, a marker of inflammation.
“Good” cholesterol, “bad” cholesterol, triglycerides! Like other blood lipids, cholesterol is not soluble in the blood. To circulate there and be delivered to cells, it needs to be carried by substances called lipoprotein. Here are the 2 main types of lipoproteins:
|
Too high or normal: how to assess cholesterol levels?
Doctors are now evaluating the cholesterol relatively. They no longer speak of normal rates but rather of rates relating to the general condition of each person and, above all, to the presence of other risk factors for maladies cardiovascular.
Thus, the cholesterol levels that an individual should aim for are estimated based on their personal rate of risk of cardiovascular diseases (angina attack, myocardial infarction, stroke) in the next 10 years. This depends on several factors: personal history of cardiovascular disease, age, smoking, diabetes, blood pressure, current total cholesterol and HDL levels, family history of cardiovascular disease, abdominal obesity, and gender.
Cardiovascular risk factors can be divided into modifiable and non-modifiable factors
Non-modifiable risk factors:
– The age of over 50 for a man or over 60 for a woman.
– Personal history of infarction or stroke,
– These same antecedents present in the first family line (sisters, brothers, father and mother) before age 55 for men and 65 for women.
Modifiable risk factors:
– low HDL-C below 0,40 g / l,
– Diabetes,
– High blood pressure,
– Smoking even if weaned for less than 3 years.
For example, for identical cholesterol levels:
- a 55 year old male smoker with hypertension will be considered at high risk. He should therefore aim to further reduce his cholesterol levels;
- a 34-year-old woman who does not smoke and does not have high blood pressure will be considered low risk: she will not need to lower her cholesterol levels as much.
Recommendations for treating cholesterol in France
Doctors use Friedewald’s formula to determine LDL-C levels (it cannot be measured in routine practice in the city lab)
LDL-C = CT – (HDL-C + TG / 5) in grams per liter
We then refer to the table below which determines the LDL-C objectives to be taken according to the associated risk factors.
What about the triglyceride level?
The rate of triglycerides varies quite easily from day to day, depending on the diet. Experts have yet to determine a target (ideal triglyceride level) for preventing heart disease. However, when the triglyceride level reaches or exceeds 1,7 mmol / l (1,5 g / l), it is a risk factor for metabolic syndrome. We are talking abouthypertriglyceridemiaabove 2 g / l.