









Contents
Craniopharyngiome
Craniopharyngioma is a rare benign tumor of the brain. As it grows, it ends up causing headaches, visual disturbances and sometimes significant hormonal disorders. A serious disease that was once fatal in children and adults, it has a much better prognosis today thanks to advances in surgery. However, the surgical intervention remains heavy and delicate … Hormonal treatments may be necessary for life.
What is craniopharyngioma?
Definition
Craniopharyngioma is a benign – that is, non-cancerous – slow-growing tumor that grows in a specific area of the brain near the pituitary gland.
Long silent, it ends up compressing brain tissue when it grows, causing signs of intracranial hypertension (headaches, eye disorders).
Depending on its extent, it can also cause other damage:
- Vision abnormalities are indicative of optic nerve damage.
- Endocrine disorders are linked to damage to the pituitary gland, the conductor of the hormonal system.
- Neurological disorders can also occur.
Causes
The uncontrolled multiplication of embryonic cells already present in the fetus is responsible for the formation of the tumor. We do not know the reason, but we know that heredity is not involved.
Diagnostic
The presence of a craniopharyngioma is suspected when its manifestations become too important to be ignored.
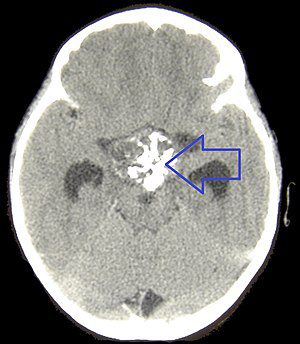
- Diagnosis is mainly based on brain imaging. MRI and CT scans can visualize the precise location of the tumor and, as a rule, distinguish it from other types of brain tumors.
- The hormonal assessment makes it possible to highlight by simple dosage in the blood deficits in growth hormone, sex hormones or thyroid hormones.
- The fluid restriction test is used to screen for diabetes insipidus. It makes it possible to assess the consequences for the patient of a total absence of drink for 5 to 15 hours. It is performed in a hospital environment.
- Examination of the fundus reveals damage to the optic nerve.
The people concerned
Craniopharyngioma is usually found in children between the ages of 5 and 15. But it sometimes develops much later, with another peak occurring between the ages of 60 and 75.
One in 50 people would be concerned. Craniopharyngioma represents less than 5% of tumors in children under 14 years old.
Symptoms of craniopharyngioma
Intracranial hypertension is manifested by intense headaches, increased by coughing or exertion. It also causes jet vomiting, independent of food intake.
Hormonal disorders are linked to damage to the pituitary gland, which produces growth hormone and various hormones that regulate secretions from other endocrine glands in the body, and releases the antidiuretic hormone made in the hypothalamus (located just above) .
- The slowdown in growth is due to a deficit in the production of growth hormone. It is a frequent sign, present in one in three children.
- Puberty is also delayed in more than half of the cases.
- In 20% of cases, the lack of antidiuretic hormone production leads to diabetes insipidus, which results in excessive urine output, frequent waking up at night to urinate or bedwetting. The child (or the adult) is thirsty all the time, he drinks a lot, otherwise he becomes dehydrated very quickly.
- Obesity, present in 10 to 25% of children at the time of diagnosis, is linked to hormonal imbalance and / or uncontrollable hunger resulting from the compression of the appetite center in the hypothalamus.
Vision disturbances can be major. Damage to the optic nerve causes a reduction in vision in one or both eyes (amblyopia) or a reduction in the field of vision due to it.
Neurological disorders sometimes appear:
- memory, learning and attention problems,
- seizures, paralysis on one side of the body or face,
- disturbances in the regulation of body temperature,
- sleeping troubles.
Treatments for craniopharyngioma
Surgical treatment
Advances in surgical techniques have offered new hope to families affected by this once fatal condition, even if some visual or neurological damage remains irreversible. The intervention aims to remove the tumor (excision) as quickly and as completely as possible.
Small craniopharyngiomas can be removed nasally, but usually it is necessary to open the skull. The intervention remains difficult, with a risk of death of between 1 and 10%.
A craniopharyngioma can be removed whole about two out of three times. In the other cases, microscopic residues prove impossible to remove and, once in ten, only part of the tumor is removed.
The recurrence rate is 35 to 70% when the excision is incomplete, and 15% when the tumor has been removed entirely.
Radiotherapy
It can be offered in the event of relapse or tumor residues, and allows 70% of patients to be permanently cured. Painless, the irradiation sessions last about fifteen minutes.
Gamma knife (radiochirurgie)
Gamma Knife radiosurgery uses very powerful gamma rays to destroy small tumors in a single irradiation.
Hormonal treatment
The pituitary gland is usually permanently damaged after the operation. Replacement hormones are administered to compensate for hormonal deficits, daily and most often for life:
- Growth hormone is prescribed for children who have stopped growing, sometimes also for adults because of its role in metabolism.
- Sex hormones allow puberty and subsequently normal sexual activity. Gonadotropin injections may also be offered to treat fertility problems.
- Thyroid hormones play a fundamental role in metabolism as well as in the development of the skeleton and nervous system.
- Desmopressin treats diabetes insipidus.
- Glucocorticoids are essential for stress management and metabolism.
Patient support
Therapeutic education
It is necessary to properly manage hormone therapy.
Psychological support
It helps to cope with the announcement of the diagnosis, the operation, the risk of relapse or the constraints of hormonal treatment.
Irrepressible appetite (overeating) is a frequent consequence of the operation, linked to damage to the hypothalamus. The incessant snacking or the food compulsions prove to be almost impossible to control, leading to weight gain sometimes significant and to psychological problems. Consulting a specialist in eating disorders can be helpful.
Specialized care
After the operation, certain disabilities require specialized follow-up.
- Up to 30% of patients have a visual handicap.
- Memory problems are also common.