









Contents
What is trisomy 18, or Edwards syndrome?
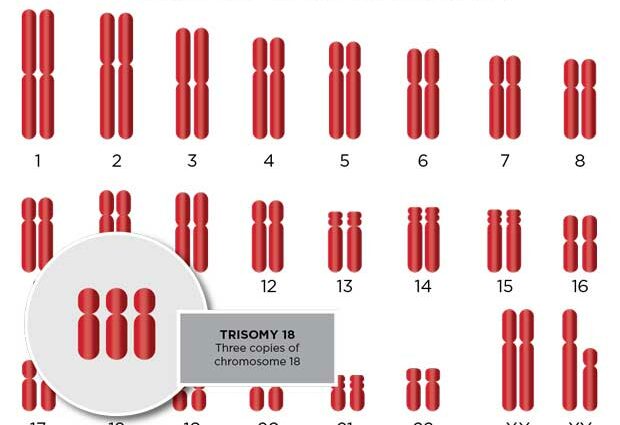
During fertilization, ovum and sperm merge to form one and the same cell, the egg-cell. This one is normally endowed with 23 chromosomes (support of the genetic inheritance) coming from the mother, and 23 chromosomes from the father. We then obtain 23 pairs of chromosomes, or 46 in total. However, it happens that an anomaly in the distribution of the genetic inheritance occurs, and that a trinomial of chromosomes is formed instead of a pair. We then speak of trisomy.
Edwards syndrome (named after the geneticist who discovered it in 1960) affects pair 18. An individual with trisomy 18 thus has three chromosomes 18 instead of two.
The incidence of trisomy 18 concerns between one in 6 births and one in 000 births, against 1 in 400 on average for trisomy 21. Unlike Down syndrome (trisomy 21), trisomy 18 results in death in utero in 95% of cases, at least according to the portal for rare diseases Orphanet.
Symptoms and prognosis of trisomy 18
Trisomy 18 is a severe trisomy, due to the symptoms it causes. Newborns with trisomy 18 present with poor muscle tone (hypotonia, which then progresses to hypertonia), hyporesponsiveness, difficulty sucking, long fingers that overlap, a upturned nose, a small mouth. Intrauterine and postnatal growth retardation is usually observed, as well as microcephaly (low head circumference), intellectual disability and motor problems. The malformations are numerous and frequent: eyes, heart, digestive system, jaw, kidneys and urinary tract… Among the other possible health concerns, we can mention a cleft lip, club feet in ice ax, ears set low, badly hemmed and angular (“faunas”) , spina bifida (neural tube closure abnormality) or a narrow pelvis.
Due to serious cardiac, neurological, digestive or renal malformations, newborns with trisomy 18 usually die in their first year of life. In the case of “mosaic” or “translocation” trisomy 18 (see below), life expectancy is longer, but does not exceed adulthood.
Because of all these health problems linked to the chromosomal abnormality, the prognosis for trisomy 18 is very unfavorable: the vast majority of affected babies (90%) die before reaching the age of one, due to complications.
Note however thatprolonged survival is sometimes possible, especially when the trisomy is partial, i.e. when cells with 47 chromosomes (including 3 chromosomes 18) coexist with cells with 46 chromosomes, including 2 chromosomes 18 (mosaic trisomy), or when chromosome 18 in addition is associated with another pair than pair 18 (translocation trisomy). But people reaching adulthood are then severely disabled, and can neither speak nor walk.
How to detect trisomy 18?
Trisomy 18 is often suspected on ultrasound, on average around the 17th week of amenorrhea (or 15th week of pregnancy), due to fetal malformations (in the heart and brain in particular), nuchal translucency too thick, growth retardation … Note that the serum markers used for screening for trisomy 21 are sometimes abnormal, but this is not always the case. Ultrasound is therefore more favorable for making the diagnosis of trisomy 18. A fetal karyotype (the arrangement of all the chromosomes) then makes it possible to confirm or not Edwards syndrome.
Trisomy 18: what treatment? What support ?
Unfortunately, there is no treatment to date to cure trisomy 18. According to the site Orphanet, surgical treatment of malformations does not significantly modify the prognosis. In addition, some malformations are such that they cannot be operated on.
The management of trisomy 18 therefore consists above all of supportive and comfort care. The goal is to improve the lives of affected babies as much as possible, by physiotherapy for example. Artificial ventilation and a gastric tube can be put in place for better nutrition and oxygenation. Management is carried out by a multidisciplinary medical team.