









Contents
Brugada syndrome
What is it ?
Brugada syndrome is a rare disease characterized by cardiac involvement. It usually results in an increased heart rate (arrhythmia). This increased heart rate can itself result in the presence of palpitations, fainting or even death. (2)
Some patients may not have any symptoms. However, despite this fact and normalcy in the heart muscle, a sudden change in the electrical activity of the heart can be dangerous.
It is a genetic pathology that can be transmitted from generation to generation.
The exact prevalence (number of cases of the disease at a given time, in a given population) is still unknown. However, its estimate is 5 / 10. This makes it a rare disease which can be fatal for patients. (000)
Brugada syndrome mainly affects young or middle-aged subjects. A male predominance is visible in this pathology, without there being an underlying poor hygiene of life. Despite this male predominance, women can also be impacted by Brugada syndrome. This greater number of men affected by the disease is explained by the different male / female hormonal system. Indeed, testosterone, an exclusively male hormone, would have a privileged role in pathological development.
This male / female predominance is hypothetically defined by an 80/20 ratio for men. In a population of 10 patients with Brugada syndrome, 8 are generally men and 2 are women.
Epidemiological studies have shown that this disease is found with a higher frequency in men in Japan and Southeast Asia. (2)
Symptoms
In Brugada syndrome, primary signs are usually visible before the onset of an abnormally high heart rate. These first signs must be identified as quickly as possible in order to avoid complications, and in particular cardiac arrest.
These primary clinical manifestations include:
- electrical abnormalities of the heart;
- palpitations;
- dizziness.
The fact that this disease has a hereditary origin and the presence of cases of this syndrome within a family may raise the question of the possible presence of the disease in the subject.
Other signs can call for the development of the disease. Indeed, nearly 1 in 5 patients suffering from Brugada syndrome have undergone atrial fibrillation (characteristic of a desynchronized activity of the heart muscle) or even present an abnormally high rate of heart rate.
The presence of fever in patients increases their risk of worsening the symptoms associated with Brugada syndrome.
In some cases, the abnormal heart rhythm may persist and lead to ventricular fibrillation. The latter phenomenon corresponds to series of abnormally rapid and uncoordinated cardiac contractions. Usually, the heart rate does not return to normal. The electrical field of the heart muscle is often impacted causing stoppages in the functioning of the heart pump.
Brugada syndrome often leads to sudden cardiac arrest and therefore to the death of the subject. The subjects affected are, in most cases, young people with a healthy lifestyle. The diagnosis must be effective quickly in order to establish rapid treatment and thus avoid lethality. However, this diagnosis is often difficult to establish from the point of view where the symptoms are not always visible. This explains the sudden death in some children with Brugada syndrome who do not show visible alarming signs. (2)
The origins of the disease
The muscle activity of the heart of patients with Brugada syndrome is normal. The anomalies are located in the electrical activity of it.
At the surface of the heart, there are small pores (ion channels). These have the ability to open and close at a regular rate to allow calcium, sodium and potassium ions to pass inside the cells of the heart. These ionic movements are then at the origin of the electrical activity of the heart. An electrical signal can then propagate from the top of the heart muscle downwards and thus allow the heart to contract and perform its role of blood “pump”.
The origin of Brugada syndrome is genetic. Different genetic mutations can be the cause of the development of the disease.
The gene most often involved in the pathology is the SCN5A gene. This gene comes into play in the release of information allowing the opening of the sodium channels. A mutation within this gene of interest causes a modification in the production of the protein allowing the opening of these ion channels. In this sense, the flow of sodium ions is greatly reduced, disrupting the beating of the heart.
The presence of only one of the two copies of the SCN5A gene makes it possible to cause a disorder in the ionic flow. Or, in most cases, an affected person has one of these two parents who have the genetic mutation for that gene.
In addition, other genes and external factors can also be at the origin of an imbalance in the level of the electrical activity of the heart muscle. Among these factors, we identify: certain drugs or an imbalance in sodium in the body. (2)
The disease is transmitted by an autosomal dominant transfer. Either, the presence of only one of the two copies of the gene of interest is sufficient for the person to develop the phenotype associated with the disease. Usually, an affected person has one of these two parents who have the mutated gene. However, in rarer cases, new mutations can appear in this gene. These latter cases concern subjects who do not have a case of the disease within their family. (3)
Risk factors
The risk factors associated with the disease are genetic.
In fact, the transmission of Brugada syndrome is autosomal dominant. Either, the presence of only one of the two copies of the mutated gene is necessary for the subject to testify to the disease. In this sense, if one of the two parents presents a mutation in the gene of interest, vertical transmission of the disease is highly probable.
Prevention and treatment
The diagnosis of the disease is based on a primary differential diagnosis. Indeed, it is following a medical examination by the general practitioner, noting the characteristic symptoms of the disease in the subject, that the development of the disease can be evoked.
Following this, a visit to a cardiologist may be recommended to confirm or not the differential diagnosis.
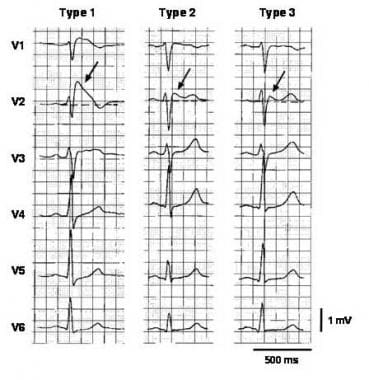
An electrocardiogram (ECG) is the gold standard in diagnosing this syndrome. This test measures the heart rate as well as the electrical activity of the heart.
In the event that Brugada syndrome is suspected, the use of drugs such as: ajmaline or even flecainide makes it possible to demonstrate an elevation of the ST segment in patients suspected of having the disease.
An echocardiogram and / or Magnetic Resonance Imaging (MRI) may be necessary to examine the possible presence of other heart problems. In addition, the blood test can measure the levels of potassium and calcium in the blood.
Genetic tests are possible to identify the possible presence of an abnormality in the SCN5A gene involved in Brugada syndrome.
The standard treatment for this type of pathology is based on the implantation of a cardiac defibrillator. The latter is similar to a pacemaker. This device makes it possible, in the event of an abnormally high beat frequency, to deliver electric shocks allowing the patient to regain a normal heart rhythm.
Currently, no drug therapy exists for the treatment of the disease. In addition, some measures can be taken to avoid rhythmic disorders. This is particularly the case with eviction due to diarrhea (impacting the sodium balance in the body) or even fever, by taking adequate drugs. (2)