









Anorexia nervosa
L’Anorexia mental is part of eating disorders or eating disorders (ADD) just like bulimia and binge eating.
The person who suffers from anorexia leads a fierce and dangerous fight against any weight gain. She is the victim of many irrational fears that can be likened to real phobias in connection with the consequences of eating, such as gaining weight or becoming obese. The result is stubborn and often dangerous food restriction.
The control exerted by people with anorexia over their diet is excessive and permanent. The appetite is most of the time preserved but the person struggles with the need and the desire for food. It requires a gradual weight loss that can go as far as emaciation (extreme thinness).
At the heart of anorexic behavior, there is a real phobia of weight gain, so intense that it pushes the person to avoid situations or behaviors that could lead to weight gain: eating unfamiliar foods, eating without doing exercise, etc. As a result, the person gradually loses weight but the satisfaction they feel is fleeting and they quickly seek to lose weight again.
The perception that she has of her body is distorted, we are talking about dysmorphophobie. These inappropriate behaviors will induce more or less serious medical complications (discomfort, panic attacks, amenorrhea, etc.) and will lead the person to become socially isolated.
Anorexia or Anorexia nervosa?
The term anorexia is misused to refer to anorexia nervosa, but anorexia nervosa is a medical entity in its own right. Anorexia is a symptom found in many pathologies (gastroenteritis, cancer, etc.) which corresponds to loss of appetite. In anorexia nervosa, the appetite is preserved but the person refuses to eat.
Causes
Anorexia nervosa is a widely studied eating disorder. The exact causes behind the onset of this disorder are complex and often intertwined.
Researchers agree to say that many factors are at the origin of anorexia including genetic, neuroendocrine, psychological, family and social factors.
Although no gene has been clearly identified, studies point to a family risk. If in the family one of its female members suffers from anorexia, there is 4 times more risk11 that another woman of this family is reached by this disorder than in a “healthy” family.
Another study conducted on identical (monozygotic) twins shows that if one of the twins suffers from anorexia, there is a 56% chance that her twin will also be affected. This probability increases to 5% if they are different twins (dizygotes)1.
Endocrine factors such as hormonal deficiency seem to be at play in this disease. The drop in a hormone (LH-RH) involved in the regulation of ovarian function is highlighted. However, this deficit is observed when there is weight loss and the LH-RH level returns to normal with weight gain. This disorder would therefore seem to be a consequence of anorexia rather than a cause.
Au neurological level, many studies put forward a serotonergic dysfunction. Serotonin is a substance which ensures the passage of the nervous message between neurons (at the level of synapses). It is particularly involved in stimulating the satiety center (area of the brain that regulates appetite). For many still unknown reasons, there is a decrease in serotonin activity in people with anorexia.2.
On the psychological level, many studies have made the link between the appearance of anorexia nervosa and a negative self-esteem (feeling of ineffectiveness and incompetence) as well as a great need for perfectionism.
Hypotheses and analytical studies find certain constants in the personality and feelings experienced by people with anorexia. Anorexia would often affect young people who avoid situations of even very low danger and who are very dependent on the judgment of others. Psychoanalytic writings often evoke a rejection of the body as a sexual object. These teenage girls would unconsciously wish they had remained little girls and would have difficulty building an identity and gaining autonomy. The disorders caused by eating disorders harm the body which “regresses” (absence of menstruation, loss of shape with weight loss, etc.).
Finally, studies carried out on the personality of people affected by anorexia, find certain types of personality more affected by this pathology such as: avoidant personality (social inhibition, feeling of not being up to the task, hypersensitivity to negative judgment. ‘others…), the dependent personality (excessive need to be protected, fear of separation,…) and the obsessive personality (perfectionism, control, rigidity, attention to detail, scrupulous attitude,…).
Au cognitive level, studies highlight automatic negative thoughts leading to false beliefs often present in anorexics and bulimics such as “thinness is a guarantee of happiness” or “any fat gain is bad”.
Finally, anorexia is a pathology that affects the population of industrialized countries more. Sociocultural factors therefore play an important place in the development of anorexia. The social criteria of beauty conveyed by young models with particularly thin and almost asexual bodies largely influence our adolescents in search of identity. The cult of thinness is omnipresent in the media, which “sells” us endlessly a profusion of miracle diets and often advocates weight control for the length of a magazine cover before, during and after the holidays and summer vacation.
Associated disorders
There are mainly psychopathological disorders associated with anorexia nervosa. However, it is difficult to know if it is the onset of anorexia that will cause these disorders or if the presence of these disorders will lead the person to become anorexic.
According to some studies3,4,5, the main psychological disorders associated with anorexia are:
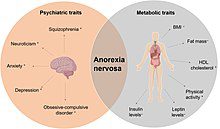
- obsessive-compulsive disorder (OCD) which affects 15 to 31% of anorexics
- social phobia
- depression that would affect 60 to 96% of anorexics at some point in the illness
Extreme fasting periods and compensatory behaviors (purges, use of laxatives, etc.) lead to complications that can cause serious kidney, heart, gastrointestinal and dental problems.
Prevalence
Described for the first time with a case study in 1689 by Richard Morton, it was not until the 50s to have a more detailed description of anorexia nervosa thanks to the important work of Hilde Bruch on this subject.
Since then, the incidence of the disease has steadily increased. According to recent studies,
the global prevalence of anorexia in the female population is estimated at 0,3%, with high mortality (between 5,1 and 13%). It would affect women 10 times more than men6,7,8.
Diagnostic
Psychopathological assessment
To make a diagnosis of anorexia nervosa, various factors must be observed in the behavior of the person.
In North America, the usual screening tool is the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) published by the American Psychiatric Association. In Europe and elsewhere in the world, healthcare professionals generally use the International Classification of Diseases (ICD-10).
In summary, to evoke an anorexic disorder, it is necessary to assess the presence of several criteria, the main one being a refusal to maintain a normal weight. Usually, the anorexic person refuses to stay at 85% of their ideal weight (obtained from height and bones). There is also an intense or even phobic fear of gaining weight associated with a significant disorder of the body diagram (distorted vision concerning weight, size and body shapes). Finally, different behaviors related to food are typical in people with anorexia such as hide food or even get others to eat. Each food intake is followed by a feeling of guilt that invades the anorexic person and leads him to adopt compensatory behavior (intensive sports practice, taking purgatives…).
Somatic assessment
In addition to the psychopathological evaluation, a complete physical examination is necessary in order to make the diagnosis of anorexia nervosa and to assess the state of undernutrition and the consequences of food deprivation on the physical health of the person.
In children under 8 years of age, the doctor will look for clues that may suggest anorexia. A slowing of the growth of stature, a stagnation or a fall in the BMI, the presence of nausea and unexplained abdominal pain will be sought.
Faced with a teenager likely to present anorexia nervosa, the specialist will look for delayed puberty, amenorrhea, physical and / or intellectual hyperactivity.
In adults, several clues may direct the doctor to a diagnosis of anorexia nervosa. Among the most common, the doctor will be vigilant in the face of weight loss (greater than 15%), a refusal to gain weight despite a low body mass index (BMI), a woman with secondary amenorrhea, a man with marked decrease in libido and erectile dysfunction, physical and / or intellectual hyperactivity and infertility.
The behaviors put in place by the person aimed at reducing food intake have more or less serious repercussions on health. The doctor will carry out a clinical and paraclinical examination (blood tests, etc.) in search of problems:
- heart problems such as heart rhythm disturbances
- dental, including erosion of tooth enamel
- gastrointestinal disorders such as bowel movement disorders
- bone, including a decrease in bone mineral density
- kidney
- dermatological
EAT-26 screening test
The EAT-26 test can screen people who may be suffering from eating disorders. This is a 26-item questionnaire that the patient fills in alone and then gives it to a professional who analyzes it. The questions will allow us to question the presence and frequency of diets, compensatory behaviors and the control that the person exercises over his eating behavior.
Source: For the French version of the EAT-26 screening test, Leichner et al. 19949
Complications
The main complications of anorexia are the more or less serious physiological disorders induced by weight loss.
In children with anorexia, severe weight loss can cause stunted growth.
The main complications of anorexia are the more or less serious physiological disorders induced by dietary restriction behaviors and purging compensators.
Dietary restrictions can lead to muscle wasting, anemia, hypotension, slowing of the heart, and low calcium levels which can lead to osteoporosis. In addition, most people with anorexia have amenorrhea (absence of periods) but this often goes unnoticed, hidden by the artificial periods created by taking the contraceptive pill.
Repeated vomiting can cause various ailments such as: erosion of tooth enamel, inflammation of the esophagus, swelling of the salivary glands and a drop in potassium levels which can cause rhythm disturbances or even heart failure. .
Taking laxatives also causes many disorders among which one can observe intestinal atony (lack of tone of the digestive tract) causing constipation, dehydration, edema and even a drop in sodium level which can lead to kidney failure.
Finally, the most serious and the most tragic of the complications of anorexia nervosa remains death by complications or suicide, which mainly affect people with chronic anorexia. The earlier anorexia is detected and managed early, the better the prognosis. Thus taken care of, the symptoms disappear in most cases over a period of 5 to 6 years after onset.