









Pioneering pulmonary artery angioplasty in chronic thromboembolic pulmonary hypertension performed for the first time in Poland at the European Health Center Otwock
On July 16, 2013, the first pulmonary artery angioplasty in patients with thromboembolic pulmonary hypertension in Poland was performed in the Department of Hemodynamics of the Department of Pulmonary Circulation and Thromboembolic Diseases of the CMKP at the European Health Center Otwock. The procedures were performed by a team of cardiologists from ECZ Otwock (Prof. Marcin Kurzyna, Prof. Adam Torbicki, Dr. Szymon Darocha) in cooperation with an interventional radiologist, Prof. Radosław Pietura from Lublin. Two patients after successful surgeries have already been discharged home.
Chronic thromboembolic pulmonary hypertension (CTEPH) is an unfavorable outcome of acute pulmonary embolism and consists in incomplete dissolution of pulmonary artery thrombi. Sometimes it is also called chronic pulmonary embolism. CTEPH results in impaired blood flow through the lungs, excessive pressure in the pulmonary artery, and development of right ventricular failure. Symptoms of heart failure include a gradual deterioration of physical capacity, shortness of breath with increasing efforts, fainting, swelling of the lower limbs, and accumulation of fluid in the pleura and peritoneum.
Symptoms of persistent exercise intolerance in a person with a history of pulmonary embolism are an indication for echocardiography, which allows for a non-invasive assessment of the pressure in the pulmonary artery. If echocardiography confirms persistent pulmonary hypertension despite anticoagulant therapy, the patient should be referred to a specialized center for the diagnosis and treatment of pulmonary hypertension. There, on the basis of imaging tests (lung perfusion scintigraphy, computed tomography, pulmonary arteriography) and cardiac catheterization, the patient undergoes the procedure of qualifying for surgery. All CTEPH patients should receive chronic anticoagulants.
It is cardiac surgery (pulmonary endarterectomy) that is the most effective method of treating CTEPH. It is a very difficult operation that requires a lot of experience of the treating team. In Poland, it is performed in centers in Warsaw (Medicover Hospital, Warszawa Wilanów) and Zabrze (Silesian Center for Heart Diseases). The perioperative mortality is about 6%, but after successful surgery, patients regain their pre-disease fitness. The condition for performing the procedure is the presence of blood clots in the large vessels of the lungs. Arteries a few millimeters in diameter are often inaccessible to the cardiac surgeon.
Unfortunately, only about 50% of patients can be treated with surgery. In the remaining patients, pharmacological treatment is applied in the same way as in the case of pulmonary arterial hypertension. In recent months, positive results of a clinical trial under the acronym CHEST were announced, which confirmed the beneficial effect of riociguat on the improvement of physical performance and hemodynamic parameters of patients with CTEPH who could not be treated surgically or in whom pulmonary hypertension persisted despite the surgery. Thus, riociguat – a representative of the new group of guanylate cyclase stimulators – is the first preparation that has a chance to obtain a registration indication for the treatment of this patient population. Until then, sildenafil remains a realistically available drug in Poland. However, it should be said that even the best pharmacological treatment is not as effective as surgery.
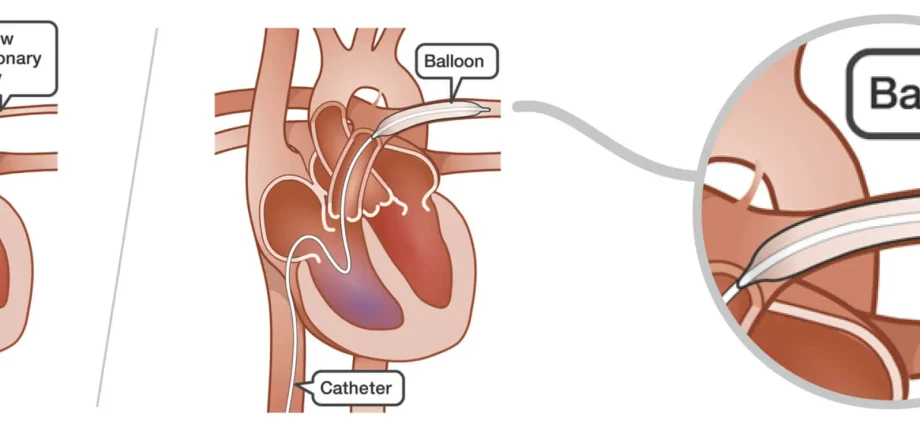
A chance for patients who cannot be operated on and supplementing pharmacotherapy is angioplasty of pulmonary arteries, ie the popular “ballooning”. This method has been used for many years in the treatment of coronary artery disease and atherosclerosis of the arteries of the lower extremities. In the lungs, it affects vessels with a diameter of 2-6 millimeters, the number of which reaches 100 in one lung. Finding vessels that qualify for angioplasty and reaching them with a balloon catheter is a real challenge for the operator. No more than two segmental vessels should dilate at a time, as this may cause swelling of the supply area in the mechanism of suddenly increased flow. Patients usually require several treatments to achieve the full effect of treatment.
The procedures are not fully financed by the National Health Fund, therefore their implementation was supported by the Pulmonary Hypertension Foundation, purchasing some of the equipment necessary to perform the procedures.
Pulmonary artery angioplasty is performed only in a few centers around the world. Now the European Otwock Health Center has joined this elite group.