









Contents
Pituitary gland
The pituitary gland (from the ancient Greek hupofusis, “outgrowth from below”) is an endocrine gland in the body located in the brain. It produces several hormones that regulate many body functions such as bone growth and the production of breast milk.
Pituitary Anatomy
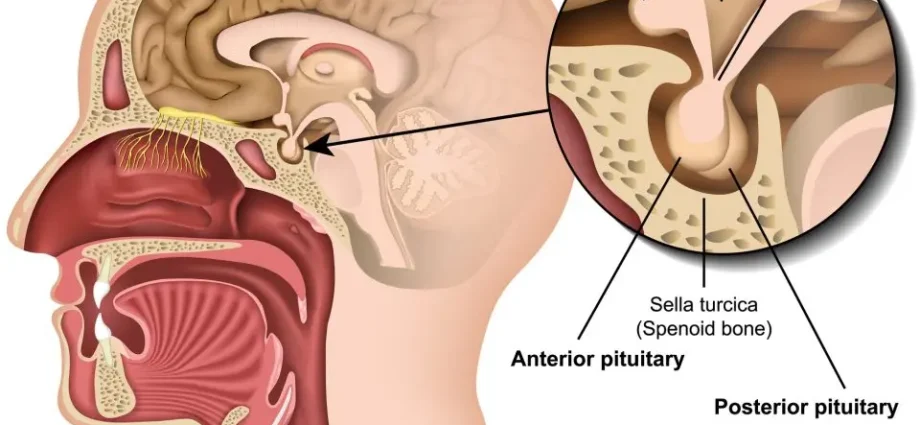
The pituitary gland, or pituitary gland, is a small endocrine gland the size of a grape that sits at the base of the brain. It is suspended from another structure, the hypothalamus, by the pituitary stem. The pituitary is made up of two lobes:
- The anterior lobe, or adenohypophysis, connected to the hypothalamus by a vascular network.
- The posterior lobe, or neurohypophysis, made up of nerve cells connected to the hypothalamus.
Pituitary physiology
The pituitary gland releases a total of eight hormones which control all hormonal secretions in the body, either directly or by acting on other glands such as the thyroid or adrenal glands. Hormones are substances which regulate a large number of essential functions (growth, pregnancy, internal temperature, adaptation and reaction to stress, to emotions, etc.).
The adenohypophysis secretes six hormones:
Name of the hormone | Target organ / Actions |
Growth hormone (GH) | Stimulates growth (especially bone and muscle growth and metabolism) |
Prolactin (PRL) | Mammary gland / Stimulates milk production |
Follicle-stimulating hormone, stimulated (FSH) | Ovaries and testes / Stimulates the production of eggs and sperm |
Luteinizing hormome (LH) | Ovary and testes / Stimulates ovulation and testosterone production |
Thyréotrophine (TSH) | Thyroid gland / Stimulates the production of thyroid hormones |
Corticotrophine (ACTH) | Kidneys (adrenal cortex) / Stimulates the secretion of glucocorticoids by the adrenal cortex |
Four of these hormones (FSH, LH, TSH and ACTH) are stimulins, that is, they act on their target organs, the endocrine glands, and stimulate them to produce hormones in turn. TSH for example, once released into the bloodstream, will stimulate the thyroid to secrete thyroid hormones.
Conversely, GH and PRL act on organs that are not endocrine glands. PRL, for example, acts directly on the mammary gland. It stimulates and maintains milk production after childbirth.
The neurohypophysis releases two hormones:
Name of the hormone | Target organ / Actions |
Oxytocin | Mammary glands and muscles of the wall of the uterus / Stimulates contraction of the uterus during childbirth and the reflex of milk secretion. |
Hormone antidiurétique (ADH) | Kidneys (renal tubules) / Promotes water reabsorption by the kidneys. |
Oxytocin and ADH are initially made by neurosecretory cells in the hypothalamus. They are then transported to the neurohypophysis where they are stored.
Regulation of hormone release
Hormones control their own release based on their concentration in the blood, this is called a feedback inhibition mechanism. As they are produced, they concentrate in the blood. The pituitary and hypothalamus are then sensitive to variations in the concentrations of these hormones. If the rate is too high, the hypothalamus stops their secretion by inhibiting the secretion of adenohypophyseal hormones by the action of inhibiting hormones. Conversely, their production is stimulated by the action of hypothalamic releasing hormones on the adenohypophysis. For example, corticoliberin (CRF) is produced by the hypothalamus to stimulate the secretion of ACTH from the adenohypophysis. The mechanism is cyclical: hormone levels decrease and increase alternately.
The release of oxytocin and ADH by the neurohypophysis is triggered by a nerve impulse from the hypothalamus.
Pituitary gland pathologies
In the event of abnormal functioning of the pituitary gland, a defect or excess production of hormones can be observed and lead to a very wide variety of endocrine pathologies. The pituitary gland is frequently the site of adenomas, benign tumors which are most often the cause of hypersecretion3,4. When the pituitary adenoma is larger than 1 cm, it is called a macroadenoma and it can lead to a lack of hormone secretion, called hypopituitarism (insufficient secretion) (5).
These adenomas can be located at the level of the different types of secreting cells of the adenohyophysis and do not have the same frequency (from the most frequent to the least frequent):
- Lactotropic adenoma, is located in the PRL secreting cells.
- Somatotropic adenoma, is located in the cells secreting GH.
- Gonadotropic adenoma, is located at the level of cells secreting FSH and LH.
- Corticotropic adenoma, is located at the level of ACTH-secreting cells.
- Thyrotropic adenoma, is located in TSH-secreting cells.
- Mixed adenoma, especially somatotropic and lactotropic, but other associations exist.
Consequences of hypersecretion (3-5):
- PRL hypersecretion: causes amenorrhea and sexual disturbances.
- Hypersecretion of GH: in children, it can lead to gigantism which results in adulthood by an exceptionally large size (the American Robert Wadlow measured 2,72 m for example). If the hypersecretion begins at the end of growth, it can cause acromegaly (among other things causes enlarged facial bones and thickening of facial tissues, sweating and joint pain).
- LH and FSH hypersecretion: does not seem to cause problems.
- Hypersecretion of ACTH: causes hypersecretion of glucocorticoids (e.g. cortisol) by the adrenal cortex, which can cause Cushing’s disease (6) (manifests as obesity with high blood pressure, diabetes and asthenia).
- ADH hypersecretion: responsible for the syndrome of inappropriate secretion of antidiuretic hormone (SIADH) which can be responsible for “water intoxication”. Characterized by a decrease in sodium level in the blood and a reduction in the volume of urine. Secretion defect caused by the presence of a cyst or tumor.
Consequences of hypopituitarism (3-5):
- Hyposecretion of GH: causes pituitary dwarfism in children. People with the disease present a reduced height which usually does not exceed 1,2 m in adulthood.
- Hyposecretion of LH and FSH: causes an absence of puberty, amenorrhea, impotence, infertility in both men and women.
- Hyposecretion of ACTH: causes a corticotropic insufficiency which is the most dangerous on the vital plan. It causes asthenia, arterial hypotension and digestive disorders.
- Hyposecretion of ADH: is the cause of diabetes insipidus. Patients suffer from polyuria (elimination of a large amount of water from their body through the urine, more than 6 liters per day) and polydipsia (excessive thirst). Treatment is possible with a synthetic hormone. Secretion defect caused by the presence of a cyst or tumor.
- Panhypopituitarism: the deficit concerns all the hormones produced by the pituitary gland.
Pituitary gland examinations and operations
Pituitary MRI: diagnostic medical examination carried out using a large cylindrical device in which a magnetic field and radio waves are produced to generate very precise images, in 2D or 3D. In the case of the pituitary gland, MRI makes it possible to highlight the presence of an adenoma responsible for the deficit in hormone secretion. It is then possible to assess the extent of the tumor and monitor its development or resorption (tumor removed by surgery).
Blood test for hormone levels: the dosage of a hormone is prescribed by the doctor in case of suspicion of a pathology. For example, a dosage of growth hormone may be requested in the case of growth disorders in children; a prolactin assay reveals hyperprolactinemia which is the cause of amenorrhea. Likewise, a TSH test can also reveal thyroid disorders. The hormone produced by the target gland can also be assayed. ACTH and cortisol can be tested at the same time and will be a good indicator of adrenal or pituitary gland damage.