









Contents
Asthma is a chronic disease, the basis of this disease is non-infectious inflammation in the airways. Both external and internal irritants contribute to the development of bronchial asthma. A number of external factors include various allergens, as well as chemical, mechanical and weather factors. This list includes both stressful situations and physical overload. The most common factor is allergy to dust.
Internal factors in the development of bronchial asthma include defects in the endocrine and immune systems, and the cause may also be bronchial reactivity and a deviation in sensitivity, this may be hereditary.
What is bronchial asthma?

Bronchial asthma is a disease of the bronchial tree of an inflammatory immune-allergic nature, characterized by a chronic, paroxysmal course in the form of broncho-obstructive syndrome and suffocation. This disease has become a really serious problem of society, as it has a progressive course. It is very difficult to heal completely.
Inflammation of the bronchi in bronchial asthma is characterized by strict specificity in comparison with other types of inflammatory processes of this localization. Its pathogenetic basis is based on an allergic component against the background of an immune imbalance in the body. This feature of the disease explains the paroxysmal nature of its course.
A host of other factors join the basic allergic component, which give bronchial asthma its characteristics:
Hyperreactivity of smooth muscle components of the bronchial wall. Any irritant effects on the bronchial mucosa end in bronchospasm;
Certain environmental factors can cause a massive release of inflammatory and allergic mediators exclusively within the bronchial tree. General allergic manifestations never occur;
The main inflammatory manifestation is mucosal edema. This feature in bronchial asthma leads to aggravation of bronchial obstruction;
Scanty mucus formation. An attack of suffocation in bronchial asthma is characterized by the absence of sputum when coughing or its scarcity;
Mainly medium and small bronchi, devoid of a cartilaginous framework, are affected;
Necessarily there is a pathological transformation of the lung tissue against the background of a violation of its ventilation;
There are several stages of this disease, which are based on the reversibility of bronchial obstruction and the frequency of asthma attacks. The more frequent and prolonged they are, the higher the stage.
In the diagnosis of bronchial asthma, they are found under the following names:
Mild or intermittent;
Moderate course or mild persistence;
Severe course or moderate persistence;
Extremely severe or severe persistent asthma.
On the basis of the above data, bronchial asthma can be characterized as a chronic sluggish inflammatory process in the bronchi, the exacerbations of which are based on a sudden onset of an attack of bronchial obstruction with suffocation, similar to an allergic reaction to environmental irritants. In the initial stages of the process, these attacks quickly arise and just as quickly stop. Over time, they become more frequent and less sensitive to treatment.
The first signs of bronchial asthma

The success of the treatment of bronchial asthma is very often determined by the timeliness of the detection of this disease.
Early signs of the disease include the following symptoms:
Shortness of breath or suffocation. They arise both against the background of complete well-being and peace at night, and during physical exertion, being in conditions of inhalation of polluted air, smoke, room dust, pollen of flowering plants, and changes in air temperature. The main thing is their suddenness in the type of attack;
Cough. Typical for an asthmatic attack is its dry type. It occurs synchronously with shortness of breath and is characterized by hoarseness. The patient, as if he wants to cough up something, but cannot do it. Only at the end of the attack, the cough can acquire a wet character, accompanied by the discharge of a meager amount of transparent sputum of the mucous type;
Rapid shallow breathing with prolonged exhalation. During an attack of bronchial asthma, patients complain not so much about difficulty in inhaling, but about the impossibility of a full exhalation, which becomes prolonged and requires great effort for its implementation;
Wheezing when breathing. They are always dry like whistling. In some cases, even remote and you can listen to them at a distance from the patient. With auscultation, they are heard even better;
Characteristic position of the patient during an attack. In medicine, this position is called orthopnea. At the same time, the patients sit down, lowering their legs, firmly grasping the bed with their hands. Such fixation of the auxiliary muscles of the limbs helps the chest in the implementation of exhalation.
Other symptoms of bronchial asthma

Bronchial asthma of any severity in the initial stages of its development does not cause general disturbances in the body. But over time, they necessarily arise, which manifests itself in the form of symptoms:
General weakness and malaise. During an attack, none of the patients is able to perform any active movements, as they increase respiratory failure. All that remains for the patient is to take the orthopnea position. In the interictal period of asthma with a mild course, the endurance of patients to physical activity is not impaired. The more severe the course of the disease, the more pronounced these violations;
Acrocyanosis and diffuse cyanosis of the skin. These symptoms characterize a severe degree of bronchial asthma and indicate the progression of respiratory failure in the body;
Tachycardia. During an attack, the number of heart contractions increases to 120-130 beats / min. In the interictal period with severe and moderate asthma, a slight tachycardia remains within 90 beats / min;
Dystrophic changes in the nails in the form of their bulging like watch glasses and distal finger phalanges in the form of thickening like drumsticks;
Signs of emphysema. This condition is typical for bronchial asthma with a long duration of the disease or a severe course. Manifested as an expansion of the chest in volume, swelling of the supraclavicular areas, expansion of the percussion pulmonary borders, weakening of breathing during auscultation;
Signs of cor pulmonale. They characterize severe bronchial asthma, which led to pulmonary hypertension in the small circle. As a result – an increase in the heart due to the right chambers, the accent of the second tone over the pulmonary valve;
Headache and dizziness. Relate to signs of respiratory failure in bronchial asthma;
Tendency to various allergic reactions and diseases (rhinitis, atopic dermatitis, psoriasis, eczema);
Causes of Asthma

There are a lot of reasons why small bronchi acquire increased irritability. Some of them act as background conditions that support inflammation and allergization, and some directly provoke an asthmatic attack. It is individual for each patient.
Hereditary predisposition. People with asthma have an increased risk of this disease in their children. An aggravated hereditary history is noted in a third of patients with asthma. This type of disease is atopic. It is very difficult to trace the factors that provoke asthma attacks. Such asthma can develop at any age, both childhood and adulthood.
Factors from the group of occupational hazards. An increase in the incidence of bronchial asthma was reliably recorded as a result of exposure to harmful production factors. It can be hot or cold air, its contamination with various small dust particles, chemical compounds and vapors.
Chronic bronchitis and infections. Viral and bacterial pathogens that cause an inflammatory process in the bronchial mucosa can provoke an increase in the reactivity of their smooth muscle components. This is evidenced by cases of bronchial asthma that occurs against the background of bronchitis with a long course, especially with signs of bronchial obstruction.
Inhaled air quality and environmental conditions. Residents of countries with a dry climate and the rural population get sick much less often than residents of industrial regions and countries with a humid and cold climate.
Smoking as a cause of asthma. Systematic inhalation of tobacco smoke leads to inflammatory changes in the mucous membrane of the bronchial tree. Therefore, every smoker is sick with chronic bronchitis. In some of them, the process is transformed into bronchial asthma. Smoking can act as a factor that maintains a constant inflammatory process and as a provocateur of each attack.
Asthma from dust. Scientists have recorded a causal relationship of room dust with the occurrence of bronchial asthma. The thing is that indoor dust is a natural habitat for house dust mites. In addition to these microscopic agents, it contains many allergens in the form of desquamated epithelial cells, chemicals and wool. Street dust becomes a provocateur of bronchial asthma only if it contains allergens: animal hair, pollen from flowers, grasses and trees. Once in the bronchial tree, they provoke a massive migration of protective immune cells into the mucous membrane, which release a large number of mediators of allergy and inflammation. The result is bronchial asthma.
Medications. Medications can sometimes be the culprit of bronchial asthma. It can be aspirin and any non-steroidal anti-inflammatory drugs. Very often, such asthma is of isolated origin with the onset of an attack only when the body comes into contact with them.
How to distinguish asthma from bronchitis?
Sometimes, differential diagnosis between bronchial asthma and bronchitis confuses even the most experienced pulmonologists. The correctness and timeliness of treatment depends on the correct interpretation of the patient’s symptoms. The differences between bronchial asthma and bronchitis are shown in the table.
Sign of the disease | Chronical bronchitis | Bronchial asthma |
Flow | Stable, sluggish with alternating periods of exacerbation and remission. The exacerbation lasts 2-3 weeks. After its relief, manifestations of the disease remain in the form of a cough. | Intermittent course in the form of sudden attacks of different duration (minutes, hours). During its occurrence, the general condition of the patient is sharply disturbed. Relief of an attack leads to a complete restoration of normal health. |
Provocation of the emergence | Hypothermia, bacterial and viral infections provoke an exacerbation in the form of an inflammatory process. Cough provocation is caused by physical exertion. | Inhalation of allergenic components with air causes an attack of bronchospasm and obstruction. Characterized by night attacks in a state of complete rest or during exercise. |
Dyspnea | Occurs exclusively with severe exacerbation or prolonged course of chronic obstructive bronchitis. | A typical and main symptom of any form and stage of the disease. Each attack is accompanied by shortness of breath. |
Cough | A constant symptom of the disease, both during its exacerbation and in remission. Has a mixed character with alternating dry and wet cough, especially in the morning. | Always dry, accompanying an attack. With its relief, a small amount of sputum is coughed up. |
Sputum | Mucopurulent, greenish-yellow or light brown, rarely transparent in large quantities. | Mucous, transparent, scanty. |
Temperature response | Occurs periodically. | Not typical. |
How to treat asthma?
The treatment of this disease is a strictly step-by-step process, which with each stage and stage of the disease must be accompanied by appropriate adjustments in terms of therapeutic measures. Only such an approach will help in the rational use of financial resources with a minimum number of side effects. After all, the main drugs for the treatment of asthma cause a lot of severe manifestations, which can be reduced by the right combination of drugs. Differentiated treatment tactics for bronchial asthma are presented in the table.
Type of medication | Basic therapy – maintenance anti-inflammatory treatment | Symptomatic therapy – relief of asthma attacks |
Asthma medications: | ||
Glucocorticosteroids | Indicated for compensated mild to moderate asthma. Significantly reduce the need for hormonal therapy (Singulair, Accolate) | Not effective in emergencies, therefore not used |
Leukotriene antagonists | Occurs exclusively with severe exacerbation or prolonged course of chronic obstructive bronchitis. | A typical and main symptom of any form and stage of the disease. Each attack is accompanied by shortness of breath. |
Monoclonal antibodies | The drug Xolair in the form of injections is indicated for the pronounced allergen component of bronchial asthma. | Not used in emergencies |
xanthines | Tablet forms: Theophylline, Neophylline, Teopec | Injection forms: high doses of aminophylline. |
Asthma inhalers: | ||
b2-agonists | Prolonged inhalers are used: Serevent, Berotek | Short-acting drugs: Salbutamol, Ventolin |
Cromons | Intal, Tailed. They are prescribed only for mild asthma. | Not effective in stopping an asthma attack |
Cholinolytics | Atrovent, Ipravent, Spiriva | Drugs are used to quickly relieve symptoms |
Glucocorticosteroids | Flixotide, Beclazon, Beclotide | Effective for relief of status asthmaticus, especially when inhaled through a nebulizer |
Combined funds | Berodual (anticholinergic ipratropium bromide + b2-agonist fenoterol) Seretide (b2-agonist salmeterol + glucocorticoid fluticasone) | Symbicort (glucocorticoid budesonide + b2-agonist formoterol. It is used by inhalation through a nebulizer. It has a very fast effect |
In the treatment of bronchial asthma, a pathogenetic approach is used. It involves the mandatory use of drugs that not only relieve the symptoms of the disease, but also turn off the mechanisms for their reappearance. In no case should one limit the use of only one adrenomimetics (salbutamol, ventolin). Unfortunately, this often happens. Patients are attracted by the quick effect of these drugs, but it will also be temporary. As the receptors of the bronchial tree become accustomed, the action of b2-agonists becomes weaker, up to its complete absence. Definitely need basic therapy.
Why do you need hormones for bronchial asthma?

Without the use of glucocorticoids, there can be no talk of controlling the disease. These funds affect the main links in the pathogenesis of asthmatic inflammation in the bronchi. They are equally effective as treatment in emergency cases, and for their prevention. Under their action, the migration of leukocyte and eosinophilic cells into the bronchial system is significantly reduced, which blocks the cascade of biochemical reactions for the release of inflammatory and allergy mediators. At the same time, the swelling of the mucous membrane decreases, the mucus becomes more liquid, which contributes to the restoration of the bronchial lumen. Do not be afraid of taking glucocorticoids. Competent selection of their dose and route of administration, combined with early treatment, is the key to maximum slowing down the progression of the disease. Due to the possibility of inhalation, the risk of systemic side effects is minimized.
New in the treatment of bronchial asthma
A relatively new direction of therapy for this disease is the use of leukotriene receptor antagonists (Glemont, Monax, Monler, Montelar, Montelukast, Singlon) and monoclonal antibodies (Xolair, Omalizumab). These drugs have already passed many clinical randomized trials and are successfully used in the treatment of many serious diseases. In relation to bronchial asthma, scientists have recorded positive effects, but discussions on the appropriateness of their use continue to be conducted.
The principle of action of these drugs is to block their connections between cellular elements during inflammation in the bronchi and their mediators. This leads to a slowdown in the ejection processes and insensitivity of the bronchial wall to action. They are not effective in the isolated treatment of bronchial asthma, therefore they are used exclusively in combination with glucocorticoids, reducing their required dose. The disadvantage of these funds is their high cost.
Diet

Diet is important to follow for faster healing. Proper nutrition is one of the basic elements in the fight against bronchial asthma. Since this disease is of an immuno-allergic nature, the diet also implies an appropriate adjustment of nutrition according to the hypoallergenic type. General nutritional rules for bronchial asthma include several points:
Prohibited Products. These include: fish dishes, caviar and seafood, fatty meats (duck, goose, pork neck), honey, beans, tomatoes and sauces based on them, yeast-based products, eggs, strawberries, citrus fruits, raspberries, currants, sweet melons , apricots and peaches, chocolate, nuts, alcohol;
Limitation of the use of dishes from premium flour and muffins, sugar and salt, fatty meat, semolina;
The basis of nutrition: hateful soups, any cereals seasoned with butter or vegetable oil, vegetable and fruit salads that do not contain prohibited foods, doctor’s sausages and sausage, chicken, rabbit, rye and bran bread, cookies (oatmeal, biscuit), sour-milk products , drinks (compotes, uzvars, teas, mineral waters);
Diet. Food is taken 4-5 times a day. Avoid overeating. Dishes can be baked, boiled, stewed, steamed. The use of fried foods and smoked meats is prohibited. The food you eat should be warm.
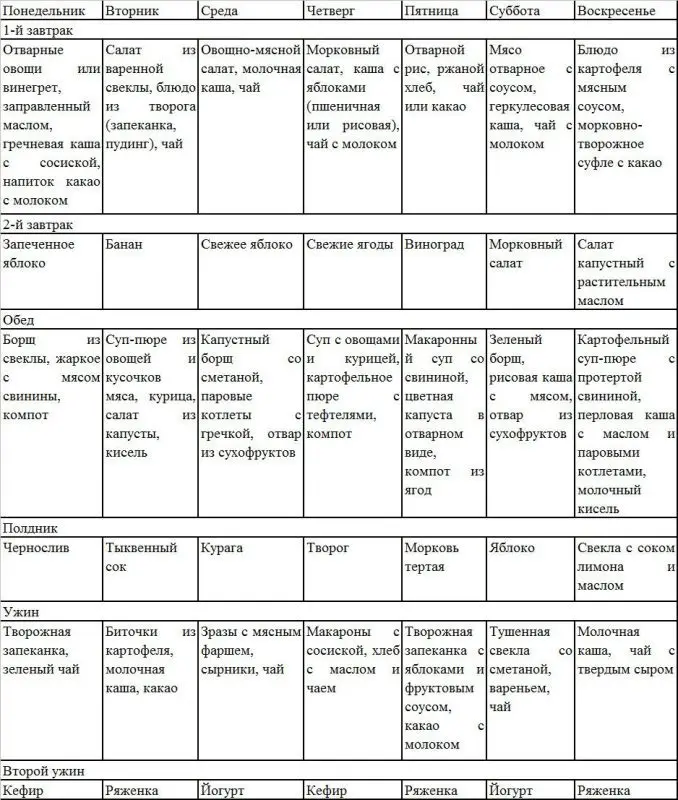
An approximate weekly menu for bronchial asthma is presented in the table.
Answers to popular questions
Can bronchial asthma be cured? It is impossible to answer this question in the affirmative with XNUMX% certainty. With all the effectiveness of treatment methods and the emergence of modern drugs, it is impossible in practice to completely eliminate the contact of a person predisposed to this disease. However, it is quite possible to control the disease and minimize its manifestations. Timely treatment, active prevention of exacerbations, accessible sports, breathing exercises will help get rid of most of the symptoms of the disease.
Is asthma hereditary? No, asthma is not a genetically determined disease, since the genes of a patient with bronchial asthma are not changed. The structural features of the respiratory system, in particular the bronchi, are genetically transmitted, as well as the increased sensitivity of the endocrine system and human immunity to irritants, that is, the body’s predisposition to the appearance of this disease. The combination of risk factors together increases the likelihood of developing asthma.
Can You Exercise With Asthma? There is no consensus among experts on this matter. On the one hand, an improperly selected sport, physical education during exacerbations can provoke bronchospasm, on the other hand, dosed physical activity normalizes metabolism, increases immunity and tone of the muscular system. This is especially important for a growing child’s body.
Can I smoke with asthma? Both active and passive smoking is absolutely incompatible with bronchial asthma, since tobacco vapors are the strongest allergens, which contain more than 4000 chemicals. Cartridges of electronic cigarettes are no less harmful for patients with bronchial asthma, as their components are able to provoke an attack. Carbon monoxide released when smoking a hookah has the same effect.
Is it possible to do inhalation with asthma? This form of administration of medicinal preparations into the body is most effective in the treatment of bronchial asthma, given the contraindications: the presence of neoplasms in the respiratory system, hyperthermia, pathology of the heart and blood vessels, diabetes mellitus, a severe form of the underlying disease, a predisposition to nosebleeds. It is important to strictly observe the dosage of essential oils and medicinal plants and fees from them, then inhalation will bring invaluable benefits.
Can I drink alcohol and coffee with asthma? Alcohol does not directly affect the respiratory system, however, its use provokes the development of inflammation, ethyl alcohol toxins negatively affect the state of all systems. In addition, most anti-asthma drugs have an incompatibility with alcohol.
Coffee, on the contrary, improves the function of the respiratory system, provided that it contains caffeine. This effect lasts 3-4 hours after drinking the drink. According to experts, coffee is a mild bronchodilator that improves the respiratory process, expanding the bronchi.
Do they take in the army with asthma? Young men with a history of bronchial asthma are not subject to conscription if this disease has passed into the second or third stages of its development, since the accumulation of sputum in the bronchi, the risk of asthma attacks upon contact with allergens, threatens not only health, but also the life of the conscript. At the first stage of the disease, the draft board gives a deferment from the call for a year or more, during which a new examination of the indicators of lung activity is carried out. A conscript’s desire to serve, backed up by improved health, may result in being offered a light duty option during which asthma treatment is continued.