









Contents
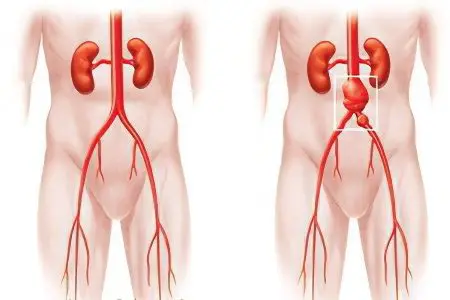
An abdominal aortic aneurysm is a bulging or diffuse expansion of the wall of the aorta located in the peritoneum. The aorta is the largest vessel in the human body. Its diameter in the abdominal region varies from 15 to 32 mm. Pathological expansion of the aortic segment can occur for a number of reasons, the main of which is atherosclerosis.
According to statistics, aneurysm of the abdominal aorta in men over 60 years of age occurs in 2-5% of cases. In children, such a pathology is observed less frequently and is predominantly congenital. In general, the prevalence of this disease is quite high. At autopsy, abdominal aortic aneurysm is diagnosed in people of both sexes in 0,6-1,6% of cases (for people over 55-60 years old). Moreover, not always the death of a person occurs precisely because of this defect in the aortic wall. But despite this, doctors put abdominal aortic aneurysm in 15th place among the most common causes of death among the population.
The problem of the development of abdominal aortic aneurysm is quite acute in cardiology and angiosurgery, since the disease threatens with serious complications, even death. However, until the moment of aneurysm rupture, a person most often does not even suspect that he has such a problem. The fact is that the aneurysm does not give itself away and can exist asymptomatically for several years. An aneurysm rupture most often ends in death, which even with timely hospitalization reaches 40%. In the postoperative period, this figure is 60% or more. Such high risks of death in patients necessitate surgical removal of the aneurysm immediately after its discovery.
Classification
There are several classifications that consider different types of peritoneal aortic aneurysm depending on its location, size, clinical course, etc.
According to the location of the peritoneal aortic aneurysm, it can be:
Suprarenal or total. This aneurysm is located above the location of the renal arteries.
infrarenal. This aneurysm is located in the aorta, below where the renal arteries originate. As a rule, such abdominal aneurysms are diagnosed in 95% of cases.
An aortic aneurysm can be:
Small – no more than 5 cm in diameter.
Middle – no more than 7 cm in diameter.
Great – more than 7 cm in diameter.
Giant – much larger than the diameter of the vessel itself.
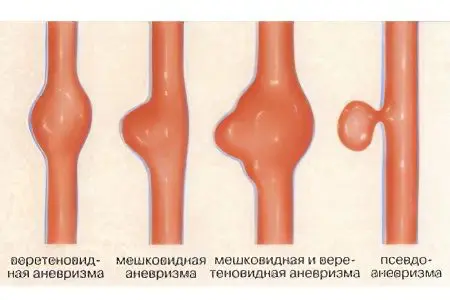
According to the form, an aneurysm located in the abdominal cavity can be of two types:
Spindle-shaped aneurysm. In this case, the aortic wall swells almost along its entire diameter.
Saccular aneurysm. Such a bulge is located on one side of the aorta, at the site of its defect. In shape, it resembles a bag with a narrow neck and a wide bottom. This sac is filled with blood.
Depending on the course of the disease, an aneurysm of the aortic peritoneum can be:
Not complicated.
Complicated by rupture, thrombosis, or delamination.
According to the structure of the protrusion wall, such aneurysms are distinguished as:
True aneurysm – this is the one that is represented by the wall of the vessel itself.
False aneurysm – this is the one that is represented by scar tissue. It replaces normal aortic tissue after a defect has occurred.
Dissecting aneurysm is a defect resulting from the divergence of the vascular wall, which is filled with blood.
What can provoke the development of an aneurysm of the aorta of the peritoneum?

Atherosclerosis is considered to be the leading cause of abdominal aortic aneurysm worldwide. Atherosclerotic vascular disease accounts for 80-90% of all cases.
Less often, various inflammatory processes act as the causes of aneurysm formation. A defect can occur against the background of pathogenic microorganisms (bacteria that cause syphilis, tuberculosis, salmonellosis, mycoplasmosis) entering the vessel wall. Rheumatic disease and nonspecific aortoarteritis sometimes act as etiological factors in the development of aneurysms.
Congenital diseases such as fibromuscular dysplasia and Marfan syndrome, as they progress, can provoke the formation of an aneurysm.
Sometimes the abdominal aorta suffers due to traumatic impact on it from the outside. A person can get similar injuries during an angiography, during an operation on the vessels. It is not excluded the formation of an aneurysm of the abdominal aorta when receiving severe bruises in the abdomen or lower back.
There are risk factors that indirectly affect the formation of a vascular wall defect.
These include:
Tobacco smoking. It has been established that 75% of patients diagnosed with peritoneal aortic aneurysm are smokers. Moreover, the longer a person smokes and the more he smokes cigarettes per day, the higher the risk that he will develop this pathology.
Belonging to the male sex and age over 55-60 years can also be attributed to risk factors for the development of this pathology.
If an abdominal aortic aneurysm was diagnosed in the next of kin, the risk of its development increases by 5 times.
Against the background of HIV infection, the risk of fungal infection of the aortic wall with the subsequent formation of an aneurysm increases.
The transferred sepsis is dangerous in this regard, when pathogenic microorganisms enter the bloodstream.
Additional risk factors are frequent stress, obesity, diabetes, malnutrition.
Separately, it is worth noting race as a risk factor for the formation of an aneurysm. It has been established that most often this pathology is diagnosed in representatives of the Caucasian race.
Hypertension, accompanied by hypertensive crises, contributes to the fact that the aortic wall will gradually wear out as a result of overstretching. As a result, a defect may form on it, which transforms into an aneurysm.
How does a peritoneal aortic aneurysm manifest itself?

If the aneurysm has an uncomplicated course, then the person will in no way suspect the presence of such a defect. This is the main insidiousness of the disease. An aneurysm may be discovered by chance during an examination for other medical conditions.
If the aneurysm reaches a large size, then it can give itself out as aching and pulling pains, which are localized in the left side or in the stomach (mainly in its lower part). Such pain is explained by the fact that the aneurysm begins to put pressure on the nerve roots of the organs located in the abdominal cavity. In this case, the pain can radiate to the back, to the lower back, to the groin. Sometimes it reaches peak values and resembles the pain that occurs against the background of acute pancreatitis or an attack of sciatica.
Often, an abdominal aortic aneurysm is disguised as a disease of the gastrointestinal tract. It can periodically manifest itself as heaviness and bloating, constipation, belching, nausea and even vomiting.
If the aneurysm is occluded by the ureter, then the patient has blood in the urine, various urination disorders occur. Large protrusions can lead to displacement of the kidney.
Suffer from the presence of an aneurysm of the aorta of the abdominal cavity of the lower limbs. A person develops ischemic disease of the legs, which is expressed in trophic lesions of soft tissues and in intermittent claudication. It is necessary to pay attention to coldness of the extremities unjustified by external factors, to numbness of the legs, accompanied by pain in the lumbar region.
Signs of a ruptured aneurysm. Against the background of a ruptured abdominal aortic aneurysm, internal bleeding can be very severe and often leads to the rapid death of the victim.
Three main symptoms that indicate a vascular catastrophe has occurred:
Severe pain in the abdomen and in the lumbar region.
Pronounced pulsation in the peritoneum.
A sudden drop in blood pressure is a collapse.
In this case, the symptoms of massive internal bleeding increase very quickly. The person turns pale, cold sweat breaks through him, weakness instantly increases, the pulse is barely audible, shortness of breath joins. If such symptoms were noticed, then it is necessary to immediately call an ambulance team. Only in this case there is a chance to save a person’s life.
Diagnostics

Sometimes it is possible to diagnose an existing defect during the examination of the patient by palpation of the peritoneum. In this case, the doctor gropes for a painful and pulsating seal. The detection of such a formation requires an immediate and more thorough examination of the patient. Instrumental methods that allow you to identify an aneurysm of the abdominal aorta are as follows:
Ultrasound of the abdominal aorta. In this case, you can see the protrusion, determine its exact location, diagnose atherosclerotic changes in the vascular wall and the presence of blood clots.
CT and MRI of the peritoneum. These two methods make it possible to clarify the location of the aneurysm and provide information on whether the daughter arteries of the aorta have undergone pathological changes.
If it is not possible to make an accurate diagnosis using ultrasound and MRI, then the patient is referred for angiography. In this case, he is injected intravenously with a contrast agent, which becomes visible under the influence of x-rays.
Abdominal x-ray can be informative in the case when calcium salts are deposited on the walls of the aneurysm. In this case, a characteristic darkening will appear in the picture.
Treatment of peritoneal aortic aneurysm

It is impossible to get rid of an abdominal aortic aneurysm with the help of drugs. Nevertheless, doctors recommend their prophylactic use in order to prevent the development of complications, and in the first place, aneurysm rupture.
Therefore, until a person has an operation, he may be prescribed the following medicines:
Drugs with cardiotropic activity – Recardium, Verapamil, Prestarium, etc.
To prevent the formation of blood clots, Warfarin, Cardiomagnyl, Clopidogrel, etc. can be prescribed.
To normalize the level of cholesterol in the blood, it is recommended to take Atorvastatin and Rosuvastatin.
Other auxiliary drugs are drugs for the treatment of diabetes mellitus, NSAIDs, antibiotics, antimycotics, etc. Their purpose depends on whether the patient has any comorbidities.
As for surgical intervention, until the moment when complications of an aortic aneurysm begin to develop in a person, it can be carried out in a planned manner. An indication for its implementation is the presence of an aneurysm of more than 5 cm in diameter. An emergency operation is performed in case of admission to the hospital of a patient with a ruptured aneurysm.
Both surgeries require general anesthesia. The patient is cut the anterior wall of the peritoneum to gain access to the aorta. Then the surgeon puts clamps on the upper and lower parts of the aneurysm, excised the pathological area and replaces it with a prosthesis. The artificial vessel itself is a tube made of synthetic materials. It takes root well in the body and does not require replacement until the end of the patient’s life. This is a complex multi-hour operation, after which the patient is sent to intensive care.
High-tech surgical interventions include endovascular stenting procedure. In this case, an incision in the abdominal cavity is not required, and the stent itself is inserted into the aorta, blocking the existing defect from the inside. The stent enters the vessel through the femoral artery. The whole procedure is carried out under the control of x-ray television. This method is not widely used in Russia due to its high cost and the need to manufacture a custom-made stent.
Prognosis of the disease
If an abdominal aortic aneurysm is left untreated, it threatens the development of serious complications that will definitely lead to the death of the patient. Here are the hard statistics: an aneurysm rupture of 5-9 cm in diameter occurs in 75% of patients during the year. If the size of the aneurysm does not reach 5 cm, then the risk of its rupture during the year decreases to 5%. Moreover, after an aneurysm rupture, 100% of patients die without medical assistance, and after the operation, no more than 10% of patients survive after the first two months.
If the operation is carried out in a planned manner, then the five-year survival rate of such patients is about 70%, which is very encouraging for people with a diagnosed aneurysm.