









Eustachian tube
The Eustachian tube (named after the Italian Renaissance anatomist Bartolomea Eustachio), now called the ear tube, is a canal connecting the middle ear to the nasopharynx. It can be the site of various pathologies having repercussions on good hearing.
Anatomy
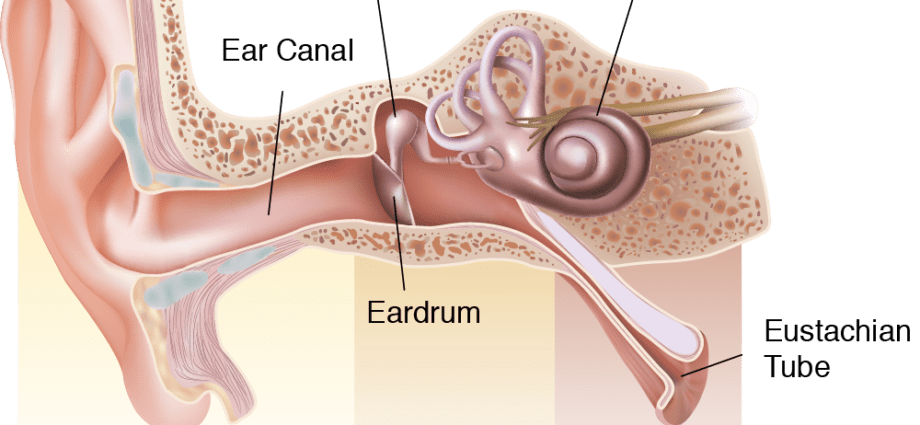
Made up of a posterior bony segment and an anterior segment of a fibro-cartilaginous nature, the Eustachian tube is a canal slightly curved upwards, measuring approximately 3 cm long and 1 to 3 mm in diameter at age adult. It connects the middle ear (formed by the tympanic cavity and the tympano-ossicular chain made up of the 3 ossicles) to the upper part of the throat, the nasopharynx. It opens laterally behind the nasal cavity.
physiology
Like a valve, the eustachian tube opens during swallowing and yawning. It thus makes it possible to circulate the air in the ear and to maintain the same pressure on both sides of the tympanic membrane, between the inner ear and the outside. It also ensures the ventilation of the middle ear as well as the drainage towards the throat of the secretions of the ear, thus avoiding the accumulation of serous secretions in the cavity of the eardrum. Through its functions of equipressure and immune and mechanical protection, the Eustachian tube contributes to the physiological integrity and proper functioning of the tympano-ossicular system, and therefore to good hearing.
Note that the opening of the Eustachian tube can be done active as soon as the atmospheric pressure increases, by simple swallowing if the pressure variations between the body and the outside are weak, as is the case for example when descending an airplane, in a tunnel, etc., to prevent the ears do not “snap”, or by various compensatory maneuvers (Vasalva, Frenzel, BTV) when the external pressure increases rapidly, as in the freediver.
Anomalies / Pathologies
In infants and children, the eustachian tube is shorter (about 18 mm long) and straighter. The nasopharyngeal secretions therefore tend to go up to the inner ear – a fortiori without cleaning the nose or effective blowing – which can then lead to acute otitis media (AOM), characterized by inflammation of the middle ear with the presence of retrotympanic fluid. . If left untreated, otitis is accompanied by hearing loss due to the fluid behind the eardrum. This transient hearing loss can be a source, in children, of language delay, behavioral problems or academic difficulties. It can also progress to chronic otitis with, among other complications, hearing loss through perforation of the eardrum or damage to the ossicles.
Even if in adults, the eustachian tube is longer and slightly curved in shape, it is not immune to problems. The Eustachian tube opens into the nasal cavities through a small orifice which can in fact easily become blocked; its narrower isthmus can also easily become blocked. Inflammation of the lining of the nose during a cold, rhinitis or an allergic episode, adenoids, polyps in the nose, a benign tumor of the cavum can thus obstruct the eustachian tube and prevent the correct ventilation of the middle ear, resulting in typical symptoms: feeling of having the ear plugged, feeling of hearing oneself speak, clicking in the ear when swallowing or when yawning, tinnitus, etc.
Tubal dysfunction is also characterized by obstruction of the eustachian tube. This can be too thin and poorly open physiologically, without any pathology found, except for an anatomical variant. The proboscis no longer playing its role well, ventilation and pressure balancing between the middle ear and the environment no longer takes place properly, as does drainage. Serous secretions then accumulate in the tympanic cavity. It’s chronic otitis media.
Eustachian tube dysfunction can also eventually lead to the formation of a retraction pocket of the eardrum (retraction of the skin of the tympanic membrane) which can lead to hearing loss and in some cases destruction. of ossicles.
Patulous’s Eustachian tube, or tubal open bite, is a much rarer condition. It is characterized by the abnormal opening, intermittently, of the eustachian tube. The person can then hear himself speak, the eardrum playing like a resonance chamber.
Treatments
In the event of repeated acute otitis media, tympanic retraction, serum-mucous otitis with auditory repercussions and resistance to medical treatment, the installation under general anesthesia of trans-tympanic aerators, more commonly called yoyos, may be proposed. . These are systems embedded through the eardrum to provide ventilation to the middle ear.
Practiced by speech therapists and physiotherapists, tubal rehabilitation may be offered in certain cases of tubal dysfunction. These are muscle exercises and self-insufflation techniques aimed at increasing the efficiency of the muscles involved in opening the eustachian tube.
Balloon tuboplasty, or balloon tubal dilation, has been offered in some establishments for several years. This surgical intervention developed by ENT and German researcher Holger Sudhoff consists of inserting, under general anesthesia, a small catheter into the Eustachian tube, using a microendoscope. A balloon of a few 10 mm is then inserted into the tube and then delicately inflated for 2 minutes, in order to dilate the tube and thus allow better drainage of secretions. This concerns only adult patients, carriers of eustachian tube dysfunction with repercussions in the ear.
Diagnostic
To assess tubal function, the ENT doctor has various examinations:
- an otoscopy, which is a visual examination of the ear canal using an otoscope;
- audiometry to monitor hearing
- tympanometry is performed using a device called a tympanometer. It comes in the form of a soft plastic probe inserted into the ear canal. A sound stimulus is generated in the ear canal. In the same probe, a second mouthpiece to record the sound returned by the tympanic membrane in order to determine its energy. During this time, an automatic device makes it possible to vary the pressure thanks to a vacuum pump mechanism. The results are transmitted in the form of a curve. Tympanometry can be used to check the presence of fluid in the middle ear, the mobility of the tympano-ossicular system and the volume of the external auditory canal. It makes it possible to make the diagnosis, among other things, of acute otitis media, tubal dysfunction;
- nasofibroscopy;
- a scanner or IMR.